
Piles (Hemorrhoids): The Complete Management Guide
What Are Piles? Anatomy Made Simple
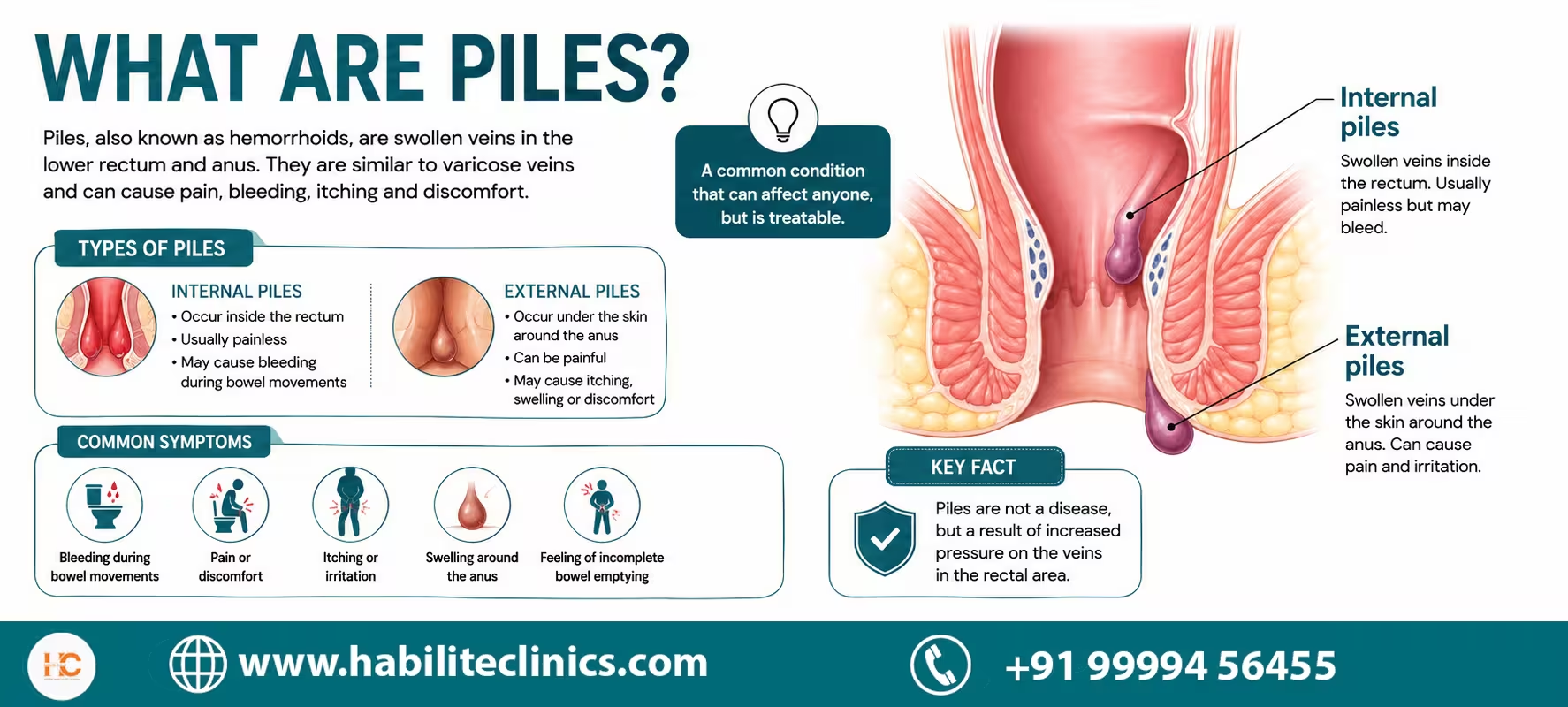
Piles, medically called haemorrhoids or hemorrhoids, are swollen, inflamed clusters of vascular tissue, smooth muscle, and connective tissue that line the anal canal. Every human being has these 'anal cushions'; they are a normal part of anal anatomy and help control continence. Piles is the term used when these cushions become symptomatic due to engorgement, prolapse, thrombosis, or bleeding.
The anal canal contains two venous plexuses:
- Internal haemorrhoidal plexus: above the dentate line; covered by insensate columnar mucosa (no pain fibres).
- External haemorrhoidal plexus: below the dentate line; covered by highly sensitive squamous epithelium (causes significant pain when thrombosed).
Key Point: The dentate line (also called pectinate line) is the anatomical boundary that determines whether a haemorrhoid is internal (painless bleeding) or external (painful, swollen lump).
If you are experiencing symptoms and want an expert assessment, consult the best laser piles surgeon in Delhi for a same-day evaluation.
How Common Are Piles? Prevalence and Risk Factors
Haemorrhoidal disease affects an estimated 4-35% of the adult population globally, making it one of the most prevalent anorectal conditions. In India, prevalence is high due to dietary patterns, sedentary work culture, and low fibre intake. Many patients self-treat for months or years before seeking specialist care.
Common Risk Factors
| Risk Factor | Why It Causes Piles |
|---|---|
| Chronic constipation | Straining increases intra-anal pressure, displacing cushions downward. |
| Low fibre diet | Hard stools cause trauma and straining. |
| Prolonged sitting / squatting | Sustained pressure on anorectal veins impairs venous return. |
| Sedentary lifestyle | Reduced bowel motility and venous stasis. |
| Pregnancy | Uterine pressure + progesterone-induced venous relaxation; constipation. |
| Obesity | Increased intra-abdominal pressure on pelvic veins. |
| Ageing | Weakening of supportive connective tissue anchoring cushions |
| Chronic diarrhoea / IBS | Repeated straining and mucosal irritation. |
| Heavy lifting | Acute Valsalva manoeuvre spikes portal venous pressure. |
| Smartphone use on toilet | Prolongs sitting time; 2025 Medscape-cited study confirmed increased risk. |
Types of Piles: Internal, External, Mixed
| Type | Where | Key Features |
|---|---|---|
| Internal | Above dentate line | Painless bright red bleeding; prolapse in advanced grades; no pain unless strangulated. |
| External | Below dentate line | Painful, especially when thrombosed; visible/palpable lump; itching and discomfort. |
| Mixed (Combined) | Both sides of dentate line | Most common presentation; exhibits features of both; often Grade III-IV at diagnosis. |
Grading of Piles (Grade I-IV)
The standard Goligher classification is used internationally to grade internal haemorrhoids and guide treatment decisions.
| Grade | Prolapse | Reduction | Preferred Treatment |
|---|---|---|---|
| I | None (only bleeds) | N/A | Diet, fibre, flavonoids, sclerotherapy |
| II | Prolapse on straining; reduces spontaneously | Spontaneous | Rubber band ligation (RBL), sclerotherapy |
| III | Prolapse requiring manual reduction | Manual only | RBL (select cases), laser haemorrhoidoplasty, DGHAL |
| IV | Permanently prolapsed; irreducible | Cannot be reduced | Excisional haemorrhoidectomy (gold standard per ASCRS 2024) |
For a detailed breakdown of the most advanced stage, read our guide on Grade 4 piles treatment, including when surgery becomes unavoidable.
Grade IV piles and symptomatic mixed (internal and external) haemorrhoids are the primary indications for excisional haemorrhoidectomy - confirmed as the most durable option by the ASCRS 2024 guidelines (Grade 1A evidence).
Upload Reports or Images for Doctor Review
Share colonoscopy, ultrasound, or even photos (if comfortable) so we can advise laser vs stapler vs medical therapy confidently.
Upload Reports or Images for Review
Share colonoscopy, ultrasonography, MRI fistulograms, or photos on WhatsApp. Dr. Kapil can plan the safest piles treatment.
👉 Tap below to open chat with our team. Attach your report (📎) and send.
Share Report on WhatsAppNeed help? WhatsApp us at +91 99994 56455
What we analyse
Each report helps us grade piles precisely and suggest the safest, quickest treatment.
- Grade and location of hemorrhoids
- Presence of fissure, fistula, or skin tag
- Pregnancy-related or post-delivery piles
- Anaemia risk from repeated bleeding
- Impact on lifestyle, travel, or office work
- Suitability for local anaesthesia vs day-care surgery
Symptoms of Piles
Many patients dismiss early piles symptoms as 'just constipation' or 'just a fissure.' Understanding the complete symptom spectrum prevents delayed diagnosis.
Internal Haemorrhoids
- Bright red blood on toilet paper or in pan (painless)
- Mucous or watery discharge causing perianal wetness and soiling
- A sensation of incomplete evacuation
- Itching and skin irritation around the anus
- Prolapse: tissue coming out during straining; may or may not reduce spontaneously
Women may experience additional symptom patterns — including pregnancy-related and postpartum piles — covered in detail in our article on symptoms of piles in women.
External Haemorrhoids
- Painful swelling or lump at the anal verge
- Acute severe pain when a clot forms (thrombosis): often described as a sharp, burning lump
- Itching, discomfort, and difficulty sitting
Red Flag Symptoms: Seek Urgent Review
Seek immediate evaluation if you experience: heavy rectal bleeding (soaking pads), fever with anal pain, inability to urinate after defaecation, blackish or dark red stools (suggests upper GI bleeding - NOT piles), significant weight loss alongside rectal bleeding, or a history of colorectal cancer in family.
Diagnosis: How We Confirm Piles
A diagnosis of haemorrhoidal disease must always be confirmed clinically. The ASCRS 2024 guidelines (Grade 1 recommendation) state: diagnosis begins with a disease-specific history and physical examination, emphasising the degree and duration of symptoms and the presence of risk factors.
Diagnostic Steps
- Detailed history: bleeding pattern, prolapse, bowel habits, diet, prior treatment.
- External inspection: identify skin tags, external haemorrhoids, soiling, excoriation.
- Digital rectal examination (DRE): assess sphincter tone, rule out masses.
- Proctoscopy / anoscopy: directly visualise internal haemorrhoids, grade prolapse, exclude anal fissure or fistula.
- Flexible sigmoidoscopy or colonoscopy: recommended for patients with rectal bleeding who are over 45 years, have a family history of colorectal cancer, or have anaemia - to exclude malignancy.
We do not diagnose piles from photos alone. Reports and photos help guide initial assessment, but a full clinical examination by a surgeon is always required before any procedure.
Non- Surgical Treatment of Piles : Diet, Lifestyle and Medication
Per ASCRS 2024 and ACG guidelines (Grade 1B evidence), dietary and behavioural modification is the primary first-line therapy for all grades of symptomatic haemorrhoids.
Dietary Recommendations
- Fibre intake: target 25-35 g/day. Psyllium husk (Isabgol) 5-10 g/day with 300 ml water is the most evidence-backed supplement for reducing bleeding and pain.
- Fluid intake: 2.5-3 litres of water daily to keep stools soft.
- Avoid straining: do not read, scroll on phone, or sit on the toilet for more than 5-7 minutes.
- Increase physical activity: 30 minutes of walking daily reduces constipation.
- Sitz baths: 10-15 minutes in warm water 2-3 times daily reduces spasm, oedema, and itching.
For a complete meal-by-meal guide tailored to Indian dietary habits, see our nutrition article on what to eat and avoid in piles
Foods to Increase
- Oats, millets (bajra, jowar), whole wheat roti
- Steamed or boiled vegetables: spinach, broccoli, bottle gourd (lauki), ridge gourd (tori)
- Fruits: papaya, guava, prunes, pear, apple with skin
- Probiotic curd (dahi): maintains healthy gut microbiome
- Warm lemon water on waking: stimulates bowel motility
Foods to Limit or Avoid
- Spicy food (chillies, hot pickles): directly irritates anal mucosa
- Deep-fried snacks (samosas, pakoras): slows bowel transit
- Maida-based foods (white bread, pastries)
- Red and processed meats
- Alcohol and carbonated drinks: cause dehydration and constipation
Beyond diet, there are several evidence-based habits that reduce flare-up frequency — see how to prevent piles with home remedies for a practical daily routine.
Medications Used in Conservative Management
| Class | Example Drugs | Mechanism / Notes |
|---|---|---|
| Phlebotonics (Flavonoids) | Diosmin-Hesperidin (Daflon), MPFF | ASCRS 2024 updated guidelines highlight this class as underutilised; reduces venous engorgement and bleeding. Grade 2B evidence. |
| Fibre supplements | Psyllium husk (Isabgol), methylcellulose | First-line; bulks stool, reduces straining. Grade 1A evidence. |
| Topical anaesthetics | Lignocaine gel, Lidocaine ointment | Short-term symptomatic relief for external pain; not curative. |
| Stool softeners | Lactulose, PEG (Polyethylene glycol) | Reduce straining; useful post-procedure and perioperatively. |
| Topical steroids | Hydrocortisone suppositories | Short course reduces inflammation; do not use more than 2 weeks (risk of mucosal atrophy). |
| Calcium dobesilate | Doxium | Reduces capillary permeability; used for acute bleeding episodes. |
Office-Based (Non-Surgical) Procedures
These are day-care procedures requiring no general anaesthesia, no hospitalisation, and minimal recovery time. They are effective for Grade I, II, and selected Grade III internal haemorrhoids.
Rubber Band Ligation (RBL): ASCRS 2024 First Choice
A small rubber band is placed at the base of each internal haemorrhoid above the dentate line, cutting off its blood supply. The haemorrhoid shrivels and falls off within 5-7 days. The ASCRS 2024 guidelines designate RBL as the most effective office-based procedure (Grade 1A evidence). One retrospective study of 2,635 patients showed 86.7% symptom-free at 8 weeks, with 15.5% recurrence at 2 years requiring repeat banding or surgery.
- Best for: Grade I, II, and select Grade III internal haemorrhoids
- Can be repeated if needed
- Rare but serious complication: perineal sepsis - fever, severe anal pain, and urinary difficulty after banding are emergency warning signs requiring immediate antibiotics and examination under anaesthesia
For Grade II–III haemorrhoids where RBL is insufficient, laser piles treatment in Delhi at Habilite Clinics offers a day-care alternative with minimal downtime.
Sclerotherapy
A sclerosing agent (typically phenol in almond oil, or polidocanol) is injected into the haemorrhoidal cushion, inducing fibrosis and reducing vascular flow. Less effective than RBL but useful when banding is not possible (e.g., anticoagulated patients).
Infrared Coagulation (IRC)
Infrared light generates heat, causing coagulation and fibrosis of the haemorrhoidal pedicle. Effective for Grade I-II; less effective than RBL for higher grades.
DGHAL / HAL (Doppler-Guided Haemorrhoidal Artery Ligation)
A proctoscope with a Doppler probe identifies feeding arteries; these are ligated with sutures, reducing blood supply to haemorrhoids. Particularly useful for Grade II-III with predominantly prolapse and bleeding. The ASCRS 2024 conditional recommendation notes: DGHAL may result in less postoperative pain than excisional haemorrhoidectomy but carries higher recurrence rates.
When to choose advanced treatment
Do You Need Laser / Stapler Surgery?
Use this quick checklist to evaluate if office procedures are sufficient or if surgery is safer.
Do symptoms persist despite medicines and high-fibre diet?
Do you have prolapse (lump coming out) or thrombosis?
Is bleeding heavy enough to cause anaemia or dizziness?
Do you need frequent hospital visits for painful flare-ups?
Has your doctor advised laser or stapler surgery earlier?
Interpretation:
Two or more “yes” responses indicate you’re likely a candidate for laser/stapler surgery. We still evaluate medically to confirm.
Need confirmation?
👉 Share your reports. We’ll suggest the safest route.
Our team reviews history, meds, and exams before recommending laser, DGHAL, stapler, or office procedures.
Prefer email? contact@habiliteclinics.com
Surgical Treatments: Indications and Technique Comparison
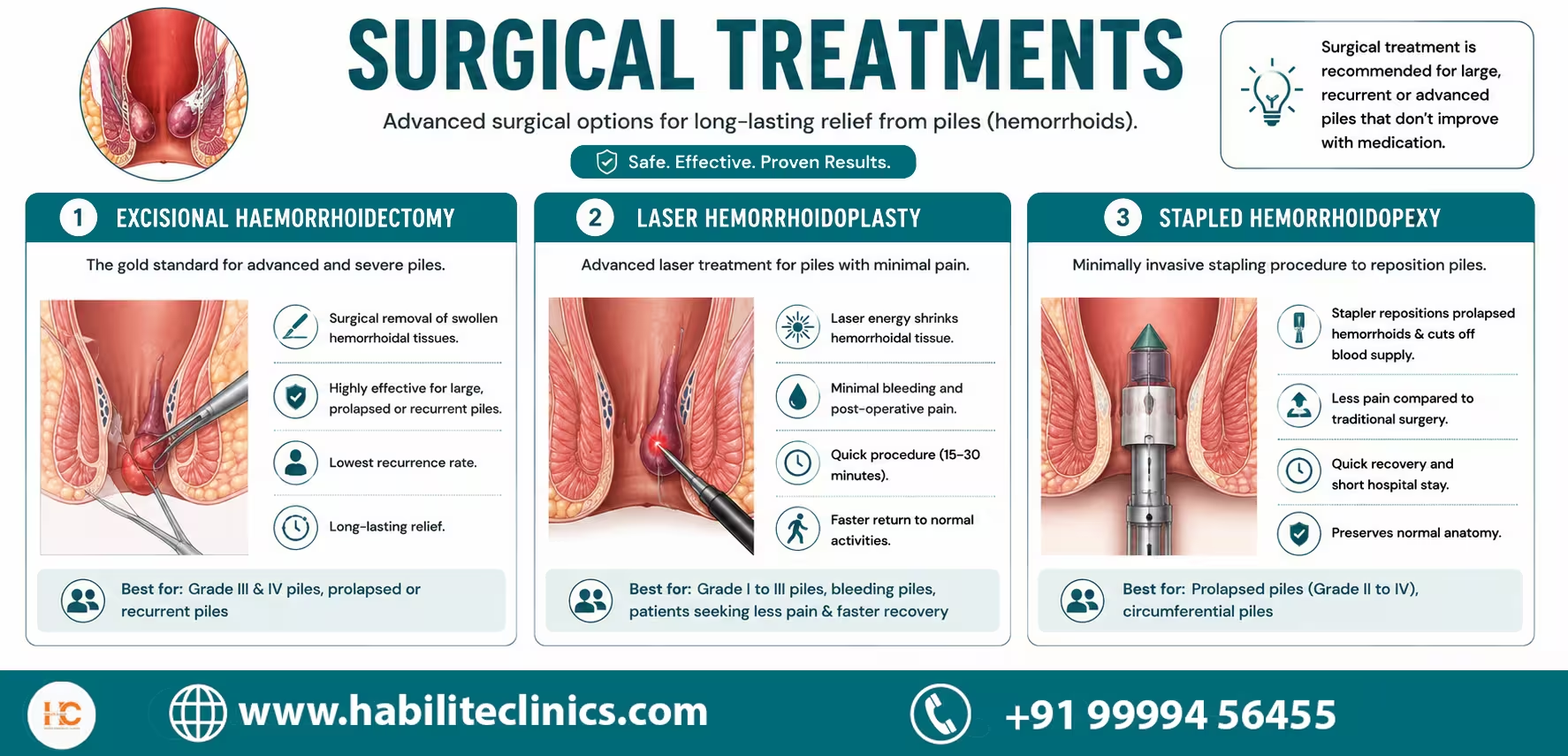
Excisional Haemorrhoidectomy: Gold Standard for Grade III-IV
The ASCRS 2024 guidelines (Grade 1A, strong recommendation) designate excisional haemorrhoidectomy as the most effective surgical treatment for Grade III-IV haemorrhoids and combined disease. Both open (Milligan-Morgan) and closed (Ferguson) techniques show equivalent outcomes.
- Recurrence rate: 2-10% (lowest of all techniques)
- Return to normal activity: 2-4 weeks
- Main downside: postoperative pain - managed with multimodal analgesia (NSAIDs, local anaesthetics, laxatives). ASCRS 2024 recommends multimodal pain regimen to reduce narcotic use (Grade 1B).
- LigaSure (vessel-sealing) haemorrhoidectomy reduces immediate postoperative pain compared to scissors or diathermy techniques.
Laser Haemorrhoidoplasty (LH)
A diode laser fibre is inserted into the haemorrhoidal pile; thermal energy causes intravascular coagulation and progressive shrinkage over 4-8 weeks without excision. Advantages include minimal pain, day-care procedure, and rapid return to work (typically 3-5 days).
- Best for: Grade II-III internal haemorrhoids
- Not suitable for: Large external component, Grade IV, or significant prolapse
- Emerging evidence: Laser haemorrhoidoplasty and radiofrequency ablation (RFA) are receiving increasing research attention as energy-based alternatives (2025 PMC review)
Stapled Haemorrhoidopexy (PPH / STARR)
ASCRS 2024 Guidance: Stapled haemorrhoidopexy has marginal efficacy as first-line surgical treatment for internal haemorrhoids AND carries a significant risk profile - therefore it is NOT routinely recommended. Evidence shows significantly higher recurrence of haemorrhoidal symptoms and prolapse compared to excisional haemorrhoidectomy. Stapling has no role in acute haemorrhoidal crisis.
Stapled haemorrhoidopexy works by resecting a mucosal cylinder above the dentate line using a circular stapler, reducing blood supply and repositioning prolapsed tissue. While associated with less postoperative pain in early trials, long-term recurrence rates are substantially higher.
Side-by-Side Treatment Comparison
| Technique | Best Grade | Pain Level | Recurrence | Recovery |
|---|---|---|---|---|
| Rubber Band Ligation | I-III | Mild | ~15% at 2 yrs | 1-2 days |
| Sclerotherapy | I-II | Nil | High | Same day |
| DGHAL / HAL | II-III | Low | Higher than EH | 3-5 days |
| Laser Haemorrhoidoplasty | II-III | Minimal | Moderate | 3-5 days |
| Excisional Haemorrhoidectomy | III-IV (Gold Standard) | Moderate-High | Lowest (2-10%) | 2-4 weeks |
| Stapled Haemorrhoidopexy | III (select) | Low | High (not recommended) | 1 week |
Gold Standard: Excisional haemorrhoidectomy is the ASCRS 2024 Grade 1A recommendation for Grade III-IV and combined internal and external disease.
Contraindications to Surgery
Not all patients with piles should undergo surgical intervention. A careful risk-benefit assessment is mandatory before any procedure.
Absolute Contraindications
These conditions preclude haemorrhoidectomy regardless of grade:
- Uncontrolled bleeding disorder (INR greater than 2.5 on anticoagulation; platelet count below 50,000 without correction)
- Portal hypertension with anorectal varices: these are NOT true haemorrhoids; standard haemorrhoidectomy can cause life-threatening haemorrhage in this setting. Hepatology evaluation is required.
- Active perianal sepsis or abscess: must be drained and treated before elective haemorrhoid surgery
- Active inflammatory bowel disease flare (Crohn's disease or ulcerative colitis in flare): any combination of IBD and haemorrhoids must be approached with extreme caution
- Inability to tolerate anaesthesia (ASA Grade IV-V without optimisation)
Relative Contraindications: Requires Case-by-Case Assessment
- Pregnancy: conservative management first; surgery only if severe complications arise. Postpartum definitive treatment is preferred.
- Immunocompromised patients (uncontrolled HIV/AIDS, neutropenia, severe uncontrolled diabetes): significantly increased risk of necrotising pelvic infection. Perioperative optimisation required.
- Faecal incontinence: surgery may worsen sphincter function; thorough anorectal physiology evaluation before proceeding.
- Prior anorectal surgery: increased risk of stricture and incontinence; careful planning and consent.
- Anticoagulation therapy: perioperative bridging plan with haematology involvement.
Special Populations
Piles in Pregnancy
Haemorrhoids are common in pregnancy due to progesterone-induced venous relaxation, uterine pressure on iliac veins, and constipation. Management is almost entirely conservative: high-fibre diet, adequate hydration, sitz baths, psyllium supplementation, and safe topical agents (lignocaine, hydrocortisone suppositories in short courses). The majority resolve postpartum. Surgery is reserved for irreducible prolapse or thrombosis with necrosis.
Elderly Patients
Ageing leads to weakening of the Parks ligament and connective tissue supporting anal cushions, making Grade III-IV more common. Frailty assessment, ASA grading, and anaesthetic fitness evaluation are essential. Day-care procedures under local or spinal anaesthesia are preferred where feasible.
Inflammatory Bowel Disease (IBD)
Both Crohn's disease and ulcerative colitis can cause anorectal symptoms that mimic or coexist with haemorrhoids. Surgery in active Crohn's perianal disease carries very high risks of non-healing wounds, fistulae, and incontinence. Always confirm IBD is in remission and obtain gastroenterology clearance before surgical intervention.
Portal Hypertension / Liver Cirrhosis
Patients with portal hypertension commonly develop anorectal varices: dilated submucosal veins that are NOT haemorrhoids. They are at risk of massive bleeding if mistakenly excised. Management is through TIPS (transjugular intrahepatic portosystemic shunt) or variceal banding, not haemorrhoidectomy.
In rare cases where pregnancy-related prolapse does not resolve postpartum, patients may require evaluation for rectal prolapse surgery in Delhi .
ASCRS 2024 and Latest Clinical Guidelines Summary
The American Society of Colon and Rectal Surgeons (ASCRS) published updated clinical practice guidelines in May 2024 (Dis Colon Rectum, 67(5):614-623). These are the most authoritative international guidelines for haemorrhoid management, reviewed by the American Academy of Family Physicians (AAFP) in December 2025.
Key 2024 ASCRS Recommendations at a Glance
| Recommendation | Grade | Evidence |
|---|---|---|
| Disease-specific history + physical exam must begin every evaluation | Strong | Low |
| Dietary modification (fibre + fluid) is first-line for all symptomatic haemorrhoids | Strong | Moderate |
| Colonoscopy is indicated for selected patients with haemorrhoidal bleeding and risk factors | Strong | Moderate |
| Rubber band ligation is the most effective office-based procedure for Grade I-III | Strong | High (1A) |
| Excisional haemorrhoidectomy is recommended for Grade III-IV and combined disease | Strong | High (1A) |
| Multimodal analgesia should be used post-haemorrhoidectomy to reduce narcotic use | Conditional | Moderate |
| Stapled haemorrhoidopexy is NOT routinely recommended - marginal efficacy, significant risk | Conditional | Moderate |
| Phlebotonics (flavonoids, MPFF) are highlighted as underutilised for symptom relief | Conditional | Moderate |
| Select thrombosed external haemorrhoids benefit from early (within 72 hrs) excision | Conditional | Low |
Emerging Trends (2024-2025 Literature)
- Radiofrequency ablation (RFA) and laser haemorrhoidoplasty: receiving increasing research attention as alternatives to IRC; 2025 PMC review notes energy-based procedures achieving haemorrhoid necrosis and fibrosis with lower complication rates.
- Digital decision-support tools: 2025 pharmacist-facing review (MDPI Pharmacy) highlights AI-assisted triage and structured algorithms improving accuracy of haemorrhoid assessment.
- Smartphone use on the toilet: 2025 Medscape-cited data confirms prolonged toilet sitting (associated with smartphone use) as an independent risk factor for haemorrhoidal disease.
- Updated quality of life metrics: newer studies incorporate disease-specific patient-reported outcomes (PROs) to guide treatment selection beyond anatomical grading alone.
Ask the Surgeon
Unsure if it’s piles, fissure, or fistula?
Describe your symptoms and we’ll respond with doctor-reviewed guidance.
Recovery, Diet and Lifestyle After Treatment
After Office Procedures (RBL / Sclerotherapy / DGHAL)
- Expect mild discomfort and a sensation of fullness for 24-48 hours after banding
- Avoid straining; take stool softeners (lactulose, PEG) for 1-2 weeks
- Light diet; increase fibre gradually
- Return to desk work: same day to 2 days
- Avoid heavy lifting and strenuous exercise for 1 week
- Sitz baths twice daily for 1-2 weeks
Patients looking for faster symptom relief during the initial recovery window can also read our article on the best way to cure piles in 3 days — covering sitz baths, diet resets, and when to escalate.
After Laser Haemorrhoidoplasty
- Mild soreness for 2-5 days; well-controlled with oral analgesics
- Resume normal diet within 24 hours; high-fibre diet maintained long-term
- Return to office work: 3-5 days
- Haemorrhoids shrink progressively over 4-8 weeks
When to See a Specialist: Red Flag Checklist
Consult a colorectal surgeon urgently if any of the following apply:
- Bright red rectal bleeding in a patient over 40 years of age: always warrants investigation
- Rectal bleeding associated with change in bowel habits or weight loss
- Anaemia, fatigue, or dizziness alongside bleeding
- A prolapsed lump that cannot be pushed back
- Severe anal pain with fever: may indicate abscess or sepsis
- Mucous or foul-smelling discharge
- Family history of colorectal cancer
- No improvement after 4 weeks of dietary change and topical medications
People also ask
FAQs about Piles & Anal Health
Expand these doctor-approved answers to understand symptoms, treatment choices, and recovery timelines.
No. Grade I and II haemorrhoids respond well to dietary changes, fibre supplements, flavonoid medications, and office-based procedures like rubber band ligation. Surgery is typically needed for Grade III haemorrhoids that fail conservative and office treatment, and for all Grade IV haemorrhoids.
Piles are swollen vascular cushions causing painless bleeding or prolapse. An anal fissure is a tear in the anal skin causing sharp pain during defaecation. An anal fistula is an abnormal tunnel between the anal canal and the skin around the anus, causing discharge and recurrent abscess. All three are separate conditions requiring different treatments, though they can coexist.
Recurrence after laser haemorrhoidoplasty is possible, particularly if lifestyle and dietary changes are not maintained. Rubber band ligation has about 15% recurrence at 2 years; excisional haemorrhoidectomy has the lowest recurrence of 2-10%. Long-term fibre intake, adequate hydration, and avoiding straining are critical to prevent recurrence.
During pregnancy we focus entirely on conservative management: high-fibre diet, sitz baths, hydration, safe topical medications, and psyllium supplements. Surgery is performed only in rare, severe cases (irreducible prolapse or thrombosis with tissue death) and requires careful multidisciplinary planning. The majority of pregnancy-related piles improve after delivery.
Recovery after excisional haemorrhoidectomy typically takes 2-4 weeks before returning to desk work. Full healing of the surgical wound takes 4-8 weeks. Laser procedures and banding involve much faster recovery, usually 3-5 days before returning to normal activity.
Excisional haemorrhoidectomy (Milligan-Morgan or Ferguson technique) is the gold standard for Grade IV piles per ASCRS 2024 guidelines (Grade 1A recommendation). It has the lowest recurrence rate of all procedures (2-10%). Laser treatment and stapling are not appropriate for Grade IV disease.
Grade I and early Grade II piles often respond to home treatment: 25-35 g dietary fibre daily, 2.5-3 litres of water, psyllium husk (Isabgol), sitz baths, and avoiding straining. However, home remedies do not cure haemorrhoids anatomically - they reduce symptoms. If bleeding persists beyond 4 weeks or a lump protrudes, a specialist consultation is necessary.
No. The ASCRS 2024 guidelines explicitly state that stapled haemorrhoidopexy has marginal efficacy as first-line surgical treatment and carries a significant risk profile - therefore it is not routinely recommended. Studies show significantly higher rates of symptomatic recurrence and prolapse compared to excisional haemorrhoidectomy. Our practice follows these guidelines: we do not offer PPH stapling as first-choice surgery.
Untreated Grade III-IV piles progressively worsen. Risks include chronic anaemia from ongoing bleeding, strangulation (a trapped prolapsed haemorrhoid losing blood supply - a surgical emergency), thrombosis causing excruciating pain, and significant impact on quality of life including work, travel, and daily activities.
Rectal bleeding has many causes. If you are over 45 years old, have a family history of colorectal cancer, or have associated symptoms like weight loss or change in bowel habits, a colonoscopy rules out polyps or cancer before attributing bleeding to haemorrhoids alone. The ASCRS 2024 guidelines recommend this for selected patients.
Diet alone can eliminate symptoms in Grade I and some Grade II haemorrhoids, but it does not remove the anatomically enlarged haemorrhoidal cushions. Think of it as management rather than cure. For Grade III-IV, dietary change reduces straining and bleeding but does not reverse prolapse or large external components.
DGHAL (Doppler-Guided Haemorrhoidal Artery Ligation) uses a Doppler ultrasound probe to identify and stitch the feeding arteries of haemorrhoids, reducing blood supply. Laser haemorrhoidoplasty uses a laser fibre inserted directly into the pile to cause thermal shrinkage. Both are minimally invasive, but DGHAL is more effective for prolapsing haemorrhoids and laser is better suited for predominantly bleeding Grade II-III piles.
Phlebotonics are a class of venoactive drugs, typically flavonoid compounds like diosmin-hesperidin (Daflon) or micronised purified flavonoid fraction (MPFF). The ASCRS 2024 guidelines updated their position on this class, noting it is underutilised in clinical practice despite evidence of benefit in reducing bleeding and acute symptoms. They are safe for most patients and are useful as an adjunct to conservative management.
The degree of pain depends on the technique. Rubber band ligation: mild discomfort for 24-48 hours. Laser: minimal pain, 2-5 days of mild soreness. Excisional haemorrhoidectomy: moderate-to-significant pain for 7-14 days, managed with a multimodal pain regimen (ASCRS 2024 Grade 1B) including NSAIDs, paracetamol, local anaesthetics, and stool softeners.
Haemorrhoids themselves do not cause or become cancer. However, rectal bleeding, the most common symptom of piles, can also be a symptom of colorectal cancer. This is why persistent rectal bleeding, especially in patients over 40, must always be evaluated by a specialist to exclude malignancy before attributing it to haemorrhoids.
A strangulated haemorrhoid occurs when a prolapsed haemorrhoid becomes trapped outside the anal canal and its blood supply is cut off. This causes severe pain, swelling, and if left untreated, tissue death (gangrene). It is a surgical emergency requiring urgent haemorrhoidectomy under general anaesthesia.
External piles feel like painful lumps at the anal opening, visible on inspection, and are particularly painful when a blood clot forms (thrombosis). Internal piles are above the dentate line - you cannot see or feel them but may notice bright red blood on tissue paper or in the toilet, and prolapse of tissue only in advanced stages. A clinical examination by a surgeon with proctoscopy is the definitive way to confirm type and grade.
After office procedures (RBL, laser): light walking is encouraged from day 1; avoid heavy lifting, intense cycling, or gym work for 2-3 weeks. After excisional haemorrhoidectomy: light walking from day 2-3; return to gym at 4-6 weeks once wound has healed and pain has settled. Yoga (avoiding inverted positions in early recovery) and walking are the best exercises during recovery.
Success stories
Patients Who Trusted Our Piles Program
Real experiences from people who chose laser, stapler, or DGHAL surgery.

Laser piles surgery with zero recurrence
Learn how laser hemorrhoidoplasty provided quick relief with minimal downtime.

Stapler surgery for Grade III piles
Patient explains painless recovery, day-care admission, and diet transition.
Videos open in YouTube.

Expert video
Piles & Anal Disorders: Causes, Grades, Treatment Roadmap
Dr. Kapil decodes hemorrhoid grades, office procedures, and when laser or stapler surgery is needed.
- • Understand symptoms, grades, and prevention
- • Learn home remedies vs clinical treatments
- • Know when to escalate to surgery
Procedure video
Laser Hemorrhoidoplasty Walkthrough
Get a behind-the-scenes view of laser piles surgery, safety checks, and healing timeline.
- • Step-by-step laser piles surgery flow
- • Recovery milestones and diet guidelines
- • Pain control and post-op hygiene tips
Technology insights
Stapler vs Laser vs DGHAL – Choosing the Right Technique
Understand pros & cons of each method and who is best suited for them.
- • Compare stapler, laser, and DGHAL outcomes
- • Cost, downtime, and anaesthesia needs
- • How we personalise technique per patient
Featured blogs
Piles Education & Home-Care Tips
Learn about modern treatments, pregnancy-safe care, and non-surgical remedies.
How to Stop Piles Bleeding at Home?
Bleeding piles or hemorrhages are swollen veins found near the rectum and anus.
How to Prevent Piles with Home Remedies?
Preventing piles at home requires a combination of healthy habits and home remedies. By taking these steps, you can reduce your risk of developing piles and enjoy better overall health and well-being. If you do develop piles, it's important to seek medical advice promptly to avoid complications and manage symptoms effectively.
Best Way to Cure Piles in 3 Days: Symptoms, Causes & Doctor-Backed Treatment
Mild, early-stage (Grade I-II) piles can see real symptom relief within 2-3 days with fibre, hydration, sitz baths and topical care — but "relief" isn't the same as "cure." Grade III-IV or thrombosed piles won't resolve permanently with home remedies alone, however consistently they're followed. Warm sitz baths plus a cold compress give the fastest pain relief; high fibre intake and hydration address the root cause. Persistent bleeding, a lump that won't shrink, or no improvement after 3 days are signs to see a doctor rather than keep self-treating. Laser treatment, DG-HAL, rubber band ligation, sclerotherapy and stapler surgery are mostly day-care, minimally invasive options once home care isn't enough. Diet and lifestyle habits that bring relief are the same ones that prevent recurrence — they need to stay consistent, not just appear during a flare-up.
Symptoms of Piles in Women: Causes, Grades, and Treatment Options
Piles — medically called haemorrhoids — are swollen veins inside or around the anus. They affect both men and women, but women face several unique triggers: pregnancy, childbirth, hormonal shifts during menstruation, and the higher rates of constipation that accompany these changes. Yet piles in women are routinely underreported because symptoms are mistaken for other gynaecological issues or simply ignored out of embarrassment. This article explains every major symptom of piles in women in plain language, why women are at higher risk, how diagnosis works, and what your treatment options look like — from simple home measures to laser surgery at a specialist clinic.
Foods to Eat and Avoid in Piles: Complete Indian Diet Guide
If you have piles — also called haemorrhoids — your diet is the single most controllable factor that decides how quickly your symptoms improve. Chronic straining during bowel movements is the primary driver of haemorrhoidal swelling, and the root cause of that straining is almost always a low-fibre diet combined with inadequate water intake. The right foods to eat in piles soften the stool, speed transit, and reduce the pressure on engorged rectal veins; the wrong foods do exactly the opposite. In this guide, Dr. Kapil Agrawal — a specialist piles surgeon in Delhi with 23+ years of experience — breaks down a practical, evidence-based Indian diet plan that you can start today.
Piles Diet & Lifestyle Cheat Sheet
Use the fibre-first mantra: hydrate, soften stool, and avoid triggers to calm flare-ups and enhance healing.
Avoid or Limit
- Deep-fried snacks
- Refined flour pastries
- Processed meat
- Spicy pickles
- Alcohol & aerated drinks
Load Your Plate With
- Warm water + lemon
- Psyllium husk with water
- Steamed veggies & salads
- Dates/prunes
- Oats & millet rotis
- Probiotic curd
WhatsApp Care Reminders
📩 Get Diet & Sitz Bath Reminders on WhatsApp
Receive daily stool-softening tips, sitz bath alerts, pain tracking prompts, and follow-up checklists straight to your phone.