Best Hernia Treatment in Delhi - A Complete Guide
Introduction
If you have noticed a bulge in your abdomen or groin that comes and goes, or a dull ache when you cough or lift something heavy, you are probably wondering the same things most of our patients wonder: Is this really a hernia? Do I need surgery? And if yes — when, and which kind?
You have come to the right place to find out. This is the same guide our team at Habilite Clinics uses to walk patients through their journey — from the first symptom to full recovery.
Dr. Kapil Agrawal is a Senior Consultant Surgeon at Apollo Hospitals, Delhi NCR, with 23+ years of experience and more than 7,000 laparoscopic and robotic procedures performed. His team treats every type of hernia — inguinal, umbilical, incisional, hiatus, femoral, epigastric, and complex recurrent hernias — using the surgical approach best suited to each patient.
Use the interactive tools below to get clarity on your own situation. You can complete a 30-second symptom self-check, share your ultrasound report for a plain-English explanation, and answer five questions that will tell you whether your hernia needs surgery now or can be safely monitored. Everything is anonymous, and our team reviews each submission personally.
Read more: What is a hernia? Causes, symptoms, and treatments →
Do You Have Hernia? Take This 30-Second Symptoms Self-Check
Your existing 7-symptom self-check is excellent. Retain exactly as-is.
Visible bulge in abdomen or groin?
Pain or discomfort in affected area?
Heaviness or pressure sensation?
Pain that worsens when standing, coughing, or straining?
Difficulty reducing the bulge?
Nausea or vomiting?
Constipation or difficulty with bowel movements?
Need Immediate Support?
👉 Share your symptoms for a personalised review.
Dr. Kapil Agrawal's hernia team will study your responses and our team will reach out to you soon.
Prefer email? contact@habiliteclinics.com
Understanding Hernia: Types We See Most Often
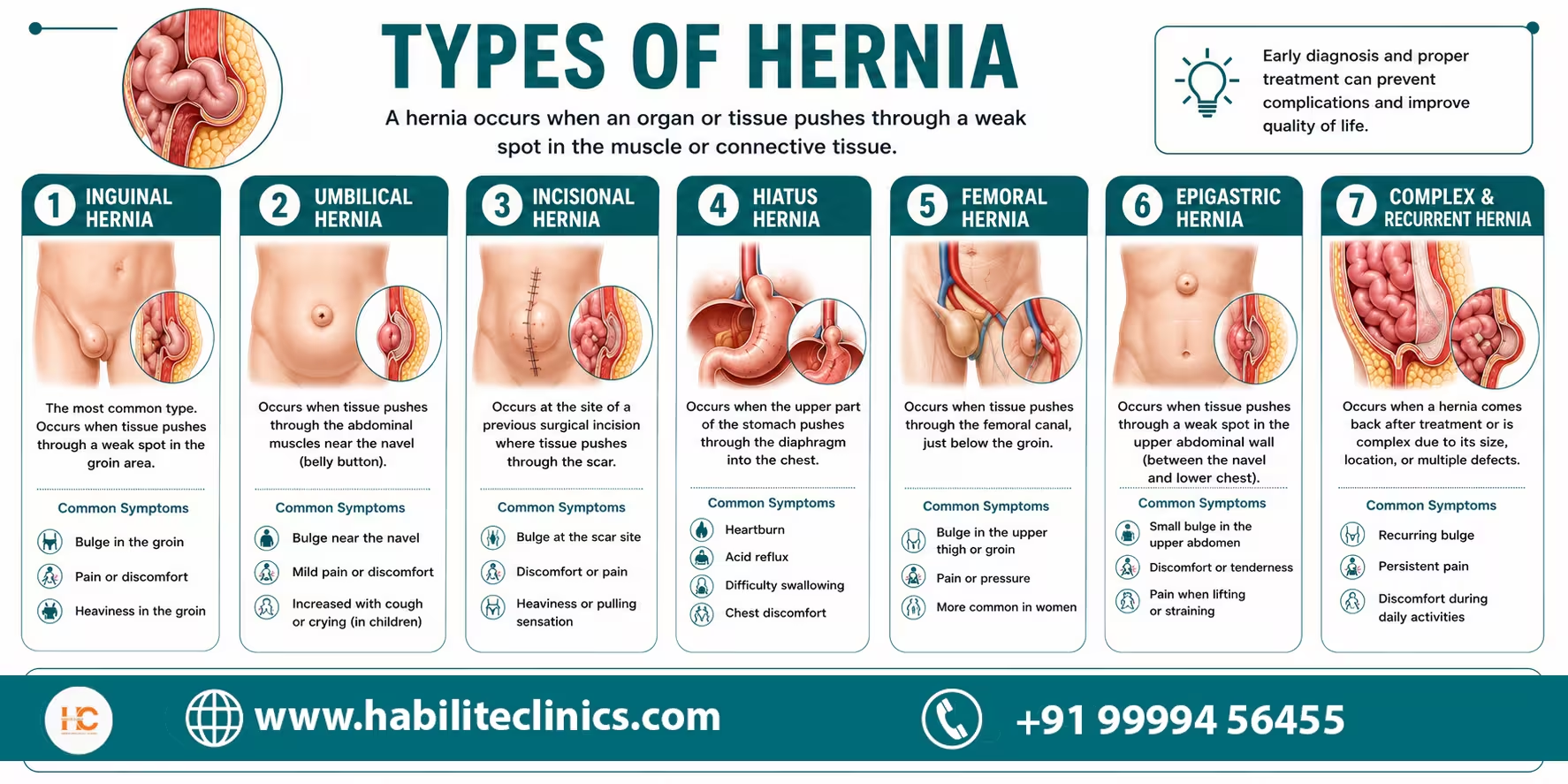
A hernia is a weak spot — a small tear or gap — in the muscle wall that holds your abdominal organs in place. When that muscle wall weakens, the organs behind it push forward and create a bulge that you can often see and feel. The type of hernia you have depends on where this weak spot is located.
Here are the seven types of hernia we treat most often at Habilite Clinics. Each one has its own typical symptoms, patient profile, and preferred surgical approach — so understanding which type you have is the first step towards the right treatment.
1. Inguinal Hernia (Groin Hernia)
This is the most common type — about 70% of all hernias are inguinal hernias. They appear as a bulge in the groin, sometimes extending into the scrotum in men. Men are 8–10 times more likely to get one than women, usually because the male groin has a natural passageway (the inguinal canal) that creates a built-in weak spot.
Typical signs: a soft lump in the groin that gets bigger when you stand, cough, or lift, and softens or disappears when you lie down; a heavy or dragging feeling; occasional sharp pain.
2. Umbilical Hernia (Belly Button Hernia)
This one pops up right around the navel. In babies, umbilical hernias are common and often close on their own by age 2–5. In adults, they appear most often during or after pregnancy, in people carrying extra weight around the abdomen, or in anyone who has had long-standing constipation or chronic cough.
Typical signs: a visible bulge at or near the belly button, soft to the touch, sometimes tender. It may look small at rest but pops out when you strain.
Read more about our Umbilical Hernia Surgery →
3. Incisional Hernia (Post-Surgical Hernia)
If you have had any abdominal surgery in the past — a C-section, appendix removal, gallbladder surgery, or anything else — there is a small chance that the healed scar later develops a weak spot. When that happens, the bulge that pushes through is called an incisional hernia.
These can appear months or even years after the original surgery. They tend to enlarge over time and are often more complex to repair than a fresh hernia, which is why we approach them with advanced imaging and a carefully planned technique.
Read more about Incisional Hernia Surgery →
4. Hiatus Hernia (Stomach Hernia)
Unlike the others, this hernia is inside your chest. Part of the stomach pushes up through an opening in the diaphragm (the breathing muscle that separates the chest from the abdomen). You cannot see or feel a hiatus hernia from the outside — but you can definitely feel its effects.
Typical signs: persistent acid reflux, heartburn that is worse after meals or when lying down, regurgitation of food, chest discomfort, difficulty swallowing, and a chronic cough that will not go away.
Read more about Hiatus Hernia & GERD Treatment →
5. Femoral Hernia
This appears lower down — in the upper thigh, just below the groin crease. Femoral hernias are much less common than inguinal hernias, but they are about four times more common in women than men. They also carry a higher risk of strangulation (where the hernia gets trapped and cuts off its own blood supply) — which is why we usually recommend repair even for small ones.
Read more about Femoral Hernia Surgery →
6. Epigastric Hernia
This one sits between the belly button and the lower end of the breastbone, along the midline of the abdomen. Epigastric hernias are usually small, but because they can cause a surprising amount of discomfort for their size, patients often come in worried that something more serious is going on.
Read more about Epigastric Hernia Surgery →
7. Complex and Recurrent Hernia
Sometimes a hernia comes back after a previous repair. Sometimes it is very large — spanning the width of the abdominal wall, with "loss of domain" (where the intestines have lived outside the abdomen for so long that bringing them back inside becomes a surgical challenge). And sometimes patients come to us after multiple previous surgeries, with scar tissue and infection making everything more complicated.
These cases are a particular focus of our practice. Dr. Kapil Agrawal and our team perform advanced techniques including Component Separation (ACS/TAR), robotic abdominal wall reconstruction, and multi-disciplinary preoperative optimisation — working alongside pulmonologists, nutritionists, and physiotherapists to give even the most difficult cases a durable, long-lasting result.
Confused About Your Hernia Ultrasound Report? We'll Explain It Clearly.
Upload your ultrasound report and receive a plain-English explanation of every finding from our medical team.
Upload Your Ultrasound Report for Explanation
PDF / JPG / PNG (max 5 MB). Share your report on WhatsApp and Dr. Kapil Agrawal's hernia team will review it.
👉 Tap below to open chat with our team. Attach your report (📎) and send.
Share Report on WhatsAppNeed help? WhatsApp us at +91 99994 56455
What we decode for you
Every term in your ultrasound can change the treatment plan. Here's what we interpret and explain in simple language.
- Hernia size and location
- Type of hernia (inguinal, umbilical, incisional)
- Contents of hernia sac
- Signs of strangulation or obstruction
- Muscle wall defect size
- Recurrence risk factors
- Mesh placement evaluation
- Post-operative healing assessment
- When surgery cannot wait
- When monitoring is possible
How Hernias Are Diagnosed
Most hernias are diagnosed the old-fashioned way — with a good physical examination. When we see you in clinic, we will ask you to stand, cough, and gently bear down while we examine the area. A clear bulge that appears when you strain and softens when you relax is usually enough to confirm the diagnosis.
But we do not stop there. An accurate diagnosis is not just about "is this a hernia" — it is about "which type, how big, what is inside it, and is it safe to wait?" To answer those questions, we often use imaging:
- Ultrasound: The first-line imaging test. Fast, painless, and accurate for most groin and umbilical hernias. We use dynamic ultrasound — where you are asked to cough or strain during the scan — to catch hernias that only appear under pressure.
- CT scan: Used for complex, recurrent, or incisional hernias where we need detailed 3D mapping of the defect, the muscle anatomy, and the hernia contents. A CT is essential before any major abdominal wall reconstruction.
- MRI: Used only occasionally, typically in athletes suspected of having a sports hernia, or when we need very detailed soft-tissue imaging.
- Endoscopy: For suspected hiatus hernia, we usually combine the clinical evaluation with an upper GI endoscopy to assess the severity of reflux and any complications in the oesophagus.
If you already have a report and are not sure what it means, use our ultrasound decoder above — our team will translate every line into plain English for you.
Surgery Necessity Checker
Do You Need Hernia Surgery? Answer These 5 Questions
This framework is what we use during clinic consultations. Answer honestly to understand whether surgery is the safer path or if monitoring is possible.
Is the hernia causing pain or discomfort?
Is the hernia enlarging over time?
Is the hernia becoming irreducible (cannot be pushed back)?
Do you have signs of strangulation (severe pain, nausea, vomiting)?
Does the hernia interfere with daily activities?
Interpreting your answers:
If you answered "Yes" to two or more questions, surgery prevents complications and improves quality of life. If all answers are "No", continue monitoring and avoid activities that increase abdominal pressure.
Need confirmation?
👉 Send your report for confirmation.
We will review your ultrasound, blood reports, and symptom history, then tell you if surgery is the safest route or if you can wait.
Prefer email? contact@habiliteclinics.com
Do I Need Surgery Now, or Can I Wait? (NEW)
This is the single most common question we hear at the first consultation: "Do I actually need surgery?" The honest answer is — it depends. And it is worth understanding exactly what it depends on, because this decision affects your next 6 months.
When surgery can often wait
For a small, painless hernia that is not growing, does not interfere with your daily life, and has no imaging signs of complication, it is often safe to monitor it — particularly if you have other medical issues that make surgery temporarily risky. In these cases, we will see you every 6–12 months, repeat the ultrasound, and help you manage daily life with practical advice on lifting, core strength, and bowel habits.
When surgery is the right call
We recommend surgical repair when any of the following are true:
- The hernia is causing pain, heaviness, or affecting your work or sleep
- It is getting larger over time
- It is becoming harder to push back in ("irreducible")
- There are any signs of strangulation — severe pain, hardness, nausea, vomiting, or fever
- You are female and have a femoral hernia (these should generally be repaired, even if small)
- You have a hiatus hernia with significant reflux that is not controlled by medication
When surgery is urgent
A hernia that suddenly becomes extremely painful, hard, discoloured, or impossible to push back — especially with nausea or vomiting — is a medical emergency. Please go to the nearest hospital immediately or call us on +91 99994 56455. Strangulated hernias are time-sensitive; treatment in the first few hours gives the best outcomes.
Treatment Options: Open, Laparoscopic, and Robotic Surgery
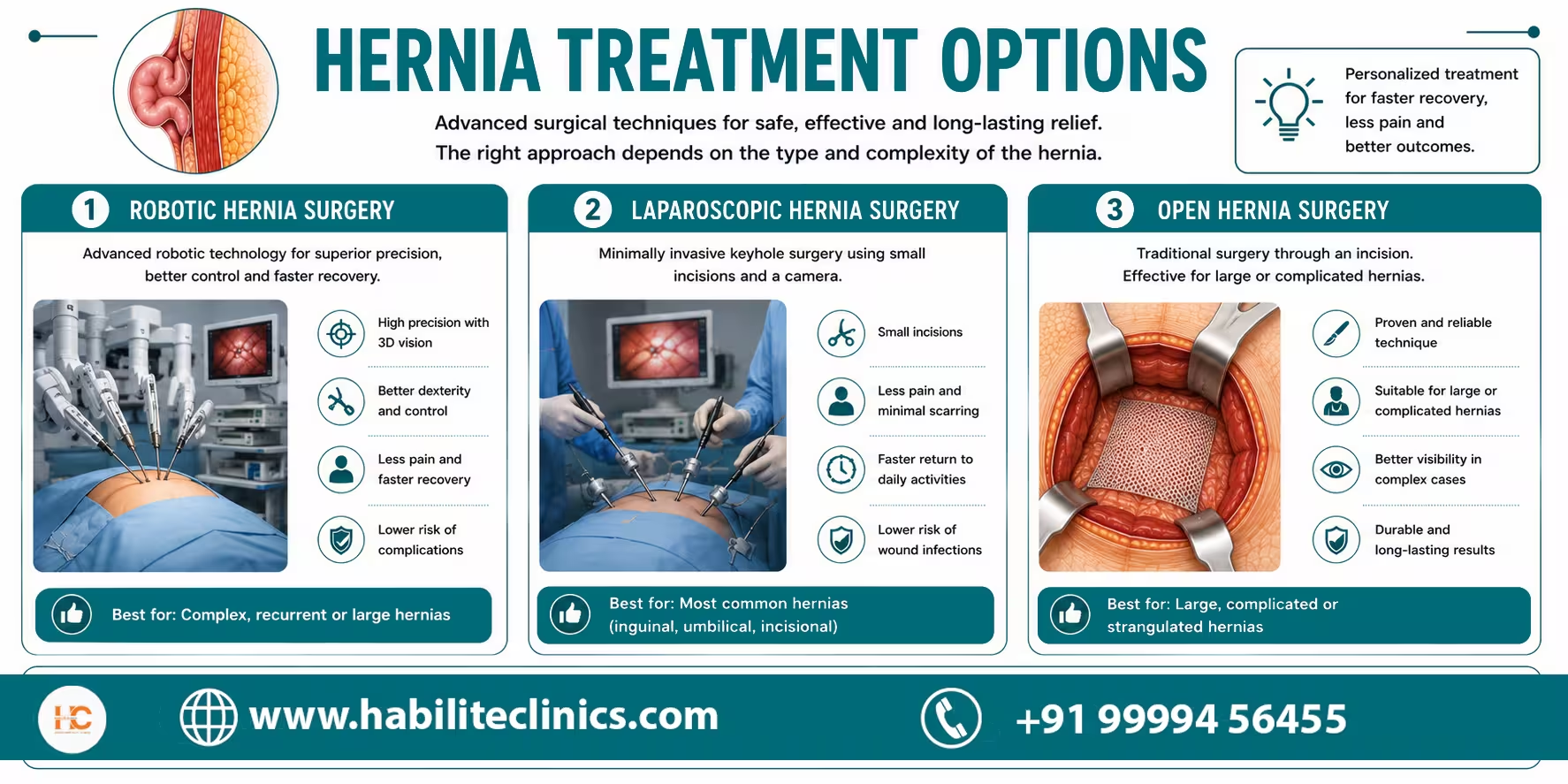
Once you and your surgeon have decided that repair is the right step, the next question is how. There are three main surgical approaches, and at Habilite Clinics we routinely perform all three. None of them is "the best" in absolute terms — the right one depends on your hernia, your body, and your life.
Laparoscopic (keyhole) hernia repair
This is the approach we use for most straightforward hernias. Instead of one large cut, we make three small incisions — each about 5 to 10 millimetres. Through these, we pass a tiny camera and slim instruments, and repair the hernia from inside the abdomen. A soft, lightweight mesh is placed to reinforce the weak area.
Why patients like it:
- Very small scars, almost invisible once healed
- Significantly less pain than open surgery
- Most patients go home the same day or within 24 hours
- Desk work in about a week, gym in 4–6 weeks
- Particularly good for bilateral (both-sided) groin hernias — we fix both through the same incisions
Robotic-assisted hernia repair
Robotic surgery takes everything good about laparoscopy and adds another layer of precision. Dr. Kapil Agrawal operates from a console a few feet from the operating table, controlling robotic arms that hold the instruments. The robot translates his hand movements with enhanced accuracy — filtering out even the smallest tremor, giving 3D magnified vision, and allowing wrist-like motion inside the body that straight laparoscopic instruments cannot achieve.
We recommend the robotic approach particularly for:
- Large or complex ventral and incisional hernias
- Recurrent hernias where there is scar tissue from a previous repair
- Abdominal wall reconstruction with component separation
- Patients who have had multiple previous abdominal surgeries
- Cases where delicate suturing in tight anatomy is required
Open hernia repair
For some patients, the classical open technique remains the right choice. We use it when:
- The hernia is very large or has strangulated and needs urgent access
- The patient cannot safely tolerate the general anaesthesia and gas-insufflation needed for laparoscopy (certain heart or lung conditions)
- There has been extensive previous abdominal surgery that makes the laparoscopic view unsafe
- The patient has specific preferences and clinical factors that favour it
Open repair uses a single incision directly over the hernia, repairs the defect, and reinforces it with mesh. Recovery is a little longer than keyhole surgery — most patients resume desk work in 2–3 weeks and full activity in 6–8 weeks.
At-a-glance comparison
| Factor | Open | Laparoscopic | Robotic |
|---|---|---|---|
| Incision size | 5–8 cm single cut | 3 × 5–10 mm keyhole | 3–5 × 5–10 mm keyhole |
| Anaesthesia | Regional or general | General only | General only |
| Hospital stay | 1–2 days typical | Same-day / 24 hours | Same-day / 24 hours |
| Pain level | Moderate | Mild | Mild |
| Return to desk work | 2–3 weeks | 5–10 dayse | 5–10 days |
| Return to gym / heavy lifting | 6–8 weeks | 4–6 weeks | 4–6 weeks |
| Scar visibility | Visible | Almost invisible | Almost invisible |
| Best for | Large / emergency / unfit for GA | Most standard hernias, bilateral groin | Complex, recurrent, large ventral |
| Relative cost | Lowest | Moderate | Highest |
Read more: Hernia surgery types, treatment options, and recovery →
Mesh vs Non-Mesh Repair
If you have spent any time reading about hernia surgery online, you will have come across worrying stories about mesh. Some of that fear is out of date — it stems from older, heavier meshes used decades ago. The modern, lightweight polypropylene meshes used today have been extensively studied, and the data is clear: for adults with a typical hernia, mesh repair reduces the recurrence rate from about 10–15% (suture-only) to 1–3% (mesh).
That said, mesh is not always the answer. We recommend non-mesh (suture-only) repair in specific situations:
- For children — where young tissue heals exceptionally well and we avoid introducing a foreign material into a growing body
- For small hernias in young, healthy adults with good tissue quality, where the defect can be repaired with confidence using sutures alone
- In emergency surgery with contamination, where placing mesh could cause infection
- In patients with documented mesh allergy (rare but real)
When we do use mesh, we choose carefully. Different mesh types are designed for different positions in the body — light for groin repairs, composite and anti-adhesive for ventral/incisional repairs where the mesh sits next to the intestine. We match the mesh to your specific anatomy.
Cost of Hernia Surgery in Delhi
The cost of hernia surgery in Delhi depends on four main factors: the type of hernia, the surgical technique used, the quality of the mesh, and the hospital category. Here is a broad range to help you plan:
Your actual cost depends on your individual case. Most patients use medical insurance (we coordinate cashless claims for almost every major insurer), and we also offer zero-interest EMI plans at our partner hospitals.
For a full cost breakdown: Complete Cost of Hernia Surgery in Delhi →
Recovery Timeline
Here is what recovery looks like for most patients after laparoscopic or robotic hernia repair. Open surgery recovery takes about twice as long at each stage.
| Timeline | What to Expect |
|---|---|
| Day 0 (surgery day) | Surgery takes 45–90 minutes. You will wake up in recovery, walk the same evening, and most patients go home within 24 hours (same day for some). |
| Days 1–3 | Mild discomfort at incision sites — well-controlled with standard painkillers. Walk regularly, eat normally, avoid lifting anything heavier than 5 kg. |
| Days 4–7 | Most patients return to desk work or light office duties. Bruising and swelling reduce. Shower normally. |
| Week 2 | Drive short distances (once comfortable without painkillers). Resume walking longer distances. Gentle stretching is fine — no core exercises yet. |
| Weeks 3–4 | Most restrictions lifted. You can begin light gym work, swim, and resume most normal activities. |
| Weeks 4–6 | Gradual return to full activity including gym, lifting, sports, and physically demanding work. By 6 weeks most patients feel completely back to themselves. |
| Month 3+ | The repair is considered fully mature. No further restrictions. |
Every recovery is individual — your age, hernia size, surgical approach, and general health all play a role. Our team stays in touch with you through structured follow-ups, and you have 24/7 WhatsApp access to us during recovery for any concern.
Warning signs that need immediate attention: sudden severe pain, high fever, expanding redness at an incision site, wound discharge, or anything that feels seriously wrong. Call us on +91 99994 56455 at any time.
Ask the Surgeon
Have A Question About Hernia Problems?
Ask Dr. Kapil Agrawal directly. Share your concern, and his team will get back to you with a personalised response.
Why Patients Across Delhi NCR Choose Dr. Kapil Agrawal
Hernia surgery is common — but that does not mean every hernia case is simple. The difference between a one-time repair and a lifetime of complications often comes down to experience.
Dr. Kapil Agrawal brings to your care:
- 23+ years of surgical experience — working full-time as a Senior Consultant Surgeon at Apollo Group of Hospitals, Delhi NCR.
- 7,000+ laparoscopic and robotic procedures — with a significant proportion being hernia repairs, including complex, recurrent, and large abdominal wall cases.
- International training — MBBS and MS from Institute of Medical Sciences BHU; MRCS from the Royal College of Surgeons, London; MMed from the National University of Singapore; FMAS in Minimal Access Surgery.
- Expertise in complex hernias — component separation (ACS/TAR), robotic abdominal wall reconstruction, recurrent hernia repair, and post-transplant hernia surgery.
- Full range of techniques available — open, laparoscopic, and robotic. We do not pick the technique based on what we prefer — we pick it based on what is best for you.
- Multi-disciplinary team — nutritionists, pulmonologists, and physiotherapists available at every stage, for every patient.
- Premium hospital infrastructure — we perform your surgery at Delhi NCR's top-tier NABH-accredited hospitals with the latest 3D/4K laparoscopic systems and robotic surgical platforms.
- Transparent, insurance-supported pricing — cashless at all major insurers, EMI options, and no hidden charges. Ever.
- Post-operative care included — structured follow-ups, 24/7 WhatsApp access to our team, nutritional guidance, and wound-care support, all at no additional cost.
People also ask
FAQs about Hernia Health
Expand each question to learn the answers Dr. Kapil Agrawal shares with his patients.
Hernias occur when an organ or fatty tissue squeezes through a weak spot in surrounding muscle or connective tissue. Common causes include congenital weakness, heavy lifting, chronic coughing, obesity, pregnancy, and previous surgeries.
Surgery is the only definitive treatment for hernias. Small, asymptomatic hernias may be monitored, but symptomatic or enlarging hernias require surgical repair to prevent complications like strangulation or obstruction.
No, hernias cannot heal on their own. The muscle wall defect will not repair itself. Surgery is necessary to fix the weakened area and prevent the hernia from enlarging or causing complications.
While small, asymptomatic hernias can sometimes be monitored, leaving a symptomatic or enlarging hernia untreated can be dangerous. It may lead to strangulation (cutting off blood supply) or obstruction, which are medical emergencies.
Avoid heavy lifting, straining during bowel movements, chronic coughing, and activities that increase abdominal pressure. Maintain a healthy weight, eat high-fiber foods to prevent constipation, and avoid smoking.
The classic sign is a soft bulge in the abdomen or groin that appears when you stand, cough, or lift something — and often disappears when you lie down. You may feel heaviness, aching, or a dragging sensation in the area. If you are unsure, use the 30-second symptom self-check at the top of this page, or share a photograph of the area on WhatsApp and our team will review it.
The seven types we treat most often are inguinal hernia (groin — the most common), umbilical hernia (around the navel), incisional hernia (at the site of a previous surgical scar), hiatus hernia (upper stomach pushing into the chest, causing reflux), femoral hernia (upper thigh, more common in women), epigastric hernia (upper abdomen above the navel), and complex or recurrent hernias (failed previous repairs or very large defects). Each type needs a slightly different surgical approach.
A general surgeon with specific experience in laparoscopic and robotic hernia repair is the right specialist. Avoid going straight to a gastroenterologist (who manages non-surgical digestive issues) or a physician (who will refer you anyway). At Habilite Clinics, Dr. Kapil Agrawal has performed over 7,000 laparoscopic and robotic procedures, including complex and recurrent hernia cases.
No. Small, painless hernias that are not growing can often be monitored for 6–12 months — we call this watchful waiting. But once a hernia causes pain, grows larger, becomes harder to push back in, or shows any sign of complication, surgery becomes the safest option. Use the 5-question Surgery Necessity Checker on this page for a quick view of where your hernia stands.
Most hernias do not stay the same size forever — they gradually enlarge over months and years, and the defect in the muscle wall keeps widening. The two serious risks of ignoring a hernia are obstruction (where intestine gets trapped and blocked) and strangulation (where the trapped tissue loses its blood supply). Both are medical emergencies. Treating a hernia electively, before complications arise, is always safer than emergency surgery.
There is no single "best" surgery — the right one depends on your hernia type, size, location, your general health, and your lifestyle. For most straightforward groin and umbilical hernias, laparoscopic (keyhole) repair gives the best balance of recovery, scarring, and outcomes. For complex, large, or recurrent hernias, robotic repair adds precision that can make a real difference. In a small number of cases, classical open surgery remains the right choice. Dr. Kapil Agrawal will discuss all three options with you.
The modern, lightweight polypropylene mesh used today is extensively studied, FDA-approved, and is the gold standard for adult hernia repair. Mesh reduces the recurrence rate from about 10–15% (sutures only) to around 1–3%. The mesh becomes integrated with your own tissue within weeks and is not felt or noticed in daily life. The older heavyweight meshes that caused some problems decades ago are no longer used at quality centres.
The cost typically ranges from Rs. 35,000 to Rs. 1,50,000 depending on the type of hernia, surgical approach, mesh used, and hospital category. Complex or robotic abdominal wall reconstructions may cost more. Most medical insurance policies in India cover hernia surgery — at Habilite Clinics, we coordinate cashless claims at all major insurers and offer zero-interest EMI options. For a full cost breakdown, see our detailed blog on hernia surgery cost in Delhi.
A straightforward laparoscopic inguinal or umbilical hernia repair takes about 45 to 60 minutes. Bilateral groin hernia repair takes 75 to 90 minutes. Complex, incisional, or recurrent hernias can take 2 to 3 hours. Most patients are discharged the same day or within 24 hours.
The surgery itself is performed under general anaesthesia, so you feel nothing during the procedure. After surgery, most patients describe the sensation as discomfort or soreness rather than pain — well-controlled with simple oral painkillers for the first 3 to 5 days. Laparoscopic and robotic repairs cause significantly less pain than traditional open surgery.
For laparoscopic or robotic repair: most patients walk the same evening, go home within 24 hours, return to desk work in 5 to 10 days, and return to full activity — gym, lifting, sports — by 4 to 6 weeks. Open surgery recovery is about twice as long at each stage. Individual recovery depends on your age, the size of the hernia, and your general health.
Most patients can drive short distances after 7 to 10 days once they are comfortable without painkillers. Desk-based office work typically resumes in 5 to 10 days after laparoscopic surgery. Physically demanding work or heavy lifting requires 4 to 6 weeks. We will give you a personalised timeline based on your job and recovery progress.
With modern mesh-based repair performed by an experienced surgeon, recurrence rates are low — about 1 to 3% over 10 years. Recurrence is more likely if you smoke, are significantly overweight, have chronic cough or constipation, return to heavy lifting too early, or had the original repair done without mesh in an adult. Following the post-operative instructions carefully is the biggest factor in preventing recurrence.
Yes. Hernia surgery is covered by almost all Indian health insurance policies, both cashless and reimbursement. Coverage typically includes surgeon is fee, hospital stay, anaesthesia, mesh, and follow-up. Our team handles insurance pre-authorisation and paperwork end-to-end, so you focus on recovery rather than forms.
Dr. Kapil Agrawal is a Senior Consultant Surgeon at Apollo Hospitals with over 23 years of experience and more than 7,000 laparoscopic and robotic procedures performed. He is qualified from IMS BHU, the Royal College of Surgeons London, and the National University of Singapore, and specialises in complex and recurrent hernia repair alongside standard hernia surgery. Our team at Habilite Clinics offers all three surgical approaches (open, laparoscopic, and robotic), personalised evaluation, transparent pricing with insurance support, and structured post-operative care at our Lajpat Nagar and Hauz Khas clinics.
Success stories
Patients Who Trusted Dr. Kapil Agrawal
Real experiences from patients who overcame hernia problems with personalised care and advanced laparoscopic surgery.
Quick Recovery After Laparoscopic Hiatus Hernia Surgery
Watch how a patient overcame years of pain with a single-stage laparscopic hernia repair and regained confidence.

Desk Job To Deadlifts In Weeks
A young executive explains her laparscopic hernia journey, from first consultation to returning to fitness training.

International Patient Undergoing Laparscopic Inguinal Hernia Repair
Detailed account of how recurrent symptoms were resolved with a tailored mesh repair and enhanced recovery.
Inguinal Hernia Repair Success Story
Hear how a senior patient experienced a pain-free, scar-conscious outcome after bilateral robotic surgery.
Videos hosted on YouTube. Clicking a card opens the testimonial in a new tab.

Expert video
Complete Hernia Treatment Journey: Evaluation, Surgery & Rehab
Dr. Kapil Agrawal explains how hernias are diagnosed, how to choose the right surgical approach, and what to expect during recovery.
- • Understand reasons behind hernia formation
- • Spot critical symptoms that need urgent evaluation
- • Compare conservative management and surgical treatment

Procedure video
How Hernia Surgery Is Done Step by Step | Complete Laparoscopic Procedure Explained
Walk through the exact steps of laparoscopic hernia repair—from anaesthesia and port placement to suturing and discharge.
- • Step-by-step overview of laparoscopic hernia repair
- • Mesh placement and hernia reduction through keyhole incisions
- • Recovery timeline, safety tips, and advantages

Technology insights
Robotic vs Laparoscopic Hernia Surgery — Which Is Better for Fast, Safe Recovery?
Dr. Kapil compares robotic precision with advanced laparoscopy, explaining how he selects the safest option for each patient.
- • Key differences in precision, incision size, pain, and recovery
- • Cost comparison and suitability for different patient conditions
- • When doctors recommend robotic surgery over laparoscopic — and why
Featured blogs
Additional Reading on Hernia Care
Dive deeper into recovery, surgery options, and financial planning with curated guides from our blog.
Hernia Surgery: Types, Treatment Options, and Recovery
Comprehensive guide to hernia surgery, including different types of hernias, treatment options, and what to expect during recovery.
Is it Safe to Delay a Hernia Surgery?
Delaying hernia surgery CAN be safe for small, asymptomatic hernias under medical supervision—but it's not risk-free According to 2025 studies, about 50-70% of patients who delay surgery eventually need it within 5-10 years Emergency complications (strangulation, incarceration) are rare but life-threatening—occurring in 2-3% of cases Delaying surgery beyond 6 months DOUBLES the risk of complications when you eventually have surgery "Watchful waiting" is an evidence-based option for specific patients—not everyone, and not indefinitely At Habilite Clinics, Dr. Kapil Agrawal helps you make informed decisions based on YOUR hernia type, symptoms, and life situation
Hernia in Children - Guidelines, Risks & Non‑Mesh Repair Guide for Parents
Hernias in children are usually congenital (present from birth) and most common in premature babies and boys Inguinal hernias (groin area) require surgery and never close on their own—they affect 1-5% of all children Umbilical hernias (belly button) often heal naturally by age 5 in 85% of small cases, but larger ones need surgical repair Mesh is NOT used in young children and our team at Habilite Clinics uses proven tissue repair methods that heal naturally Recent studies confirm mesh-free repair has excellent outcomes with only 1.3% recurrence rate in adolescents Warning signs include pain, vomiting, hard/red swelling, or a bulge that won't push back—these need immediate medical attention Most children recover within 2-3 days and can return to normal activities within one week after surgery
How to prepare for A Hernia Surgery?
Hernia repair is common and generally safe. But, as with any other procedure, preparation is crucial to prevent complications and reduce risk. Whether you are undergoing an inguinal hernia repair, umbilical hernia repair, or a different operation, what you do preoperatively is important.
Lifestyle Changes You Should Do to Manage Hernia Symptoms
Hernia is a treatable medical condition where an organ or fatty tissue protrudes, causing a visible bulge under the skin. Hernias can occur in various parts of the body, including the abdomen, groin, and upper thigh, due to aging, pregnancy, obesity, heavy lifting, chronic coughing or sneezing, or constipation.
How to Prevent Hernia?
Hernias are more common than you might suppose. If you’ve noticed a bulge in your abdomen or groin area, especially while coughing or lifting heavy objects, it could be a hernia.
Do You Have Hernia? — What to Eat & Avoid
A gentle, high-fiber diet helps prevent constipation and reduces strain. Follow these doctor-approved guidelines.
Activities to Avoid
- Heavy lifting
- Straining during bowel movements
- Chronic coughing
- Smoking
- High-fat foods
Foods to Eat
- High-fiber foods
- Fruits
- Vegetables
- Whole grains
- Lean proteins
- Plenty of water
For Personalised Diet Plan, Contact Us
📩 Enter Your WhatsApp Number
Receive the complete diet chart and weekly reminders from our clinical nutrition team.