
Best GERD & Hiatus Hernia Surgeon in Delhi, India
Dr. Kapil Agrawal offers painless laparoscopic hiatus hernia repair, tailored fundoplication, and robotic support when required. Every plan covers diagnostics, lifestyle counselling, cashless assistance, and the same enhanced recovery protocol followed for other flagship services at Habilite Clinics.
If you are searching for the best hiatus hernia treatment in Delhi, this page will walk you through everything you need to know — from what a hiatus hernia actually is, to how we diagnose it, when surgery is truly necessary, and which type of surgery is right for your specific situation.
Book Consultation
Schedule a consultation for GERD & Hiatus Hernia Surgery with Dr. Kapil Agrawal
Why Patients Choose Dr. Kapil Agrawal for Hiatus Hernia Surgery in Delhi
I understand that choosing a surgeon for something as significant as hiatus hernia surgery is not a decision you take lightly. Let me be direct about what I bring to your care:
- 23+ years of surgical experience: With a career spanning general surgery, advanced laparoscopy, robotic surgery, and bariatric procedures, I have managed the full spectrum of hiatus hernia — from straightforward sliding hernias to complex, recurrent, multi-organ paraesophageal hernias.
- International credentials: MBBS, MS Surgery, MRCS (London), MMed (Singapore). My training in the UK and Singapore exposed me to high-volume reflux surgery programmes and gave me a foundation in evidence-based surgical decision-making.
- 7,000+ minimally invasive procedures: Experience matters enormously in hiatus hernia surgery, where the quality of the cruroplasty and the precision of the fundoplication directly determine how long your repair lasts.
- Senior Consultant at Apollo Hospitals, Delhi NCR: Access to state-of-the-art operating theatres, high-definition laparoscopy, and Da Vinci robotic surgical systems.
- Founder, Habilite Clinics (Lajpat Nagar & Hauz Khas): Dedicated outpatient consultation centres focused on personalised, unhurried patient care — where your questions receive real answers, not rushed dismissals.
- Honest, patient-centred decision-making: Not every patient who comes to me needs surgery. I will tell you clearly when conservative management is the right path — and equally clearly when it is not.
What is a Hiatus Hernia?
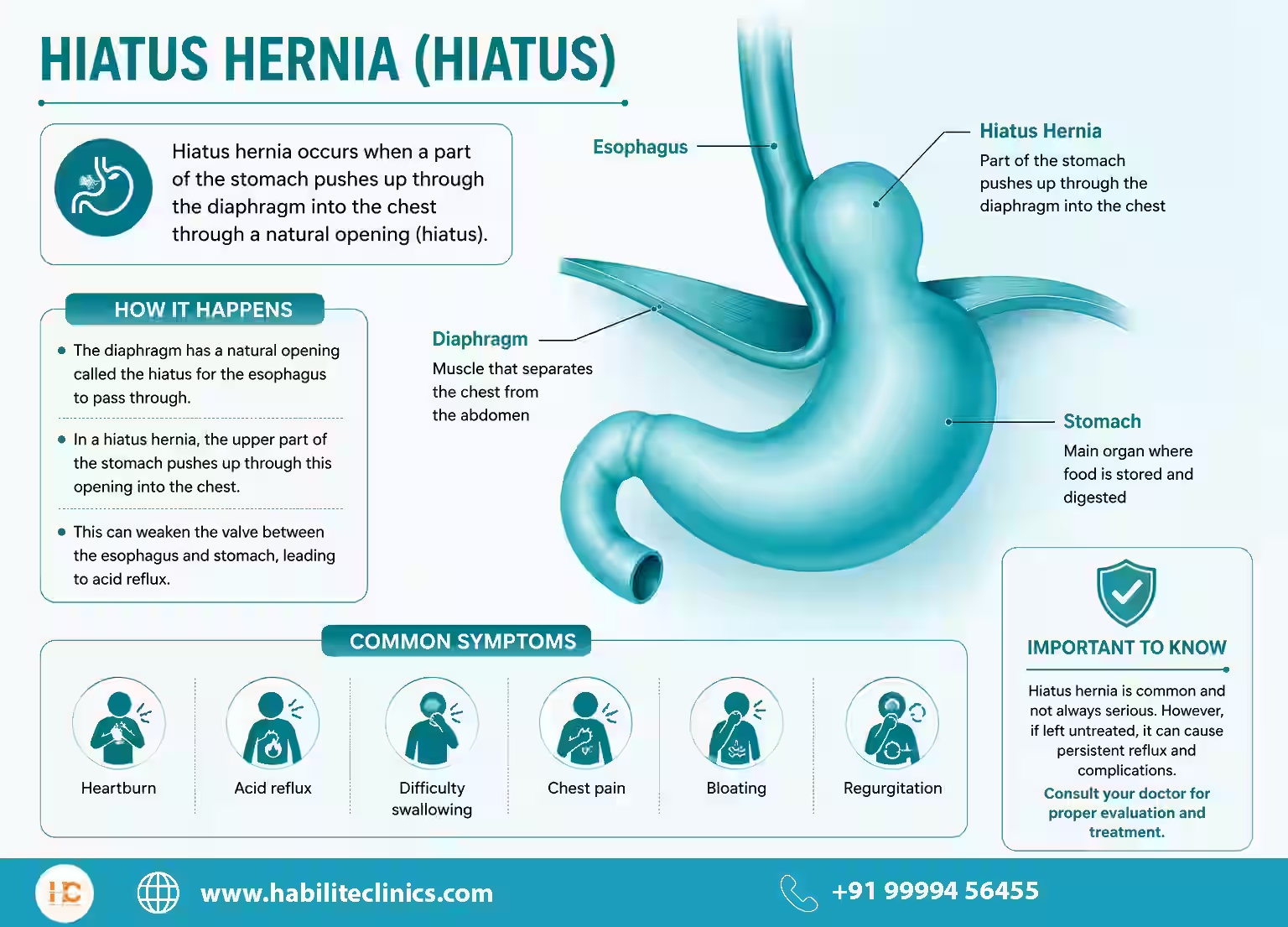
Your oesophagus (food pipe) travels from your throat down through an opening in the diaphragm — the large dome-shaped muscle that separates your chest from your abdomen — to reach the stomach. This opening is called the hiatus.
A hiatus hernia occurs when part of your stomach pushes upward through this opening into the chest cavity. This disrupts the natural valve mechanism at the junction between the oesophagus and stomach, allowing stomach acid to flow backwards into the food pipe. The result is a cascade of symptoms — heartburn, regurgitation, chest discomfort, and sometimes breathlessness — that significantly affect quality of life.
Types of Hiatus Hernia
Not all hiatus hernias are the same. Understanding the type you have is critical, because it determines the urgency of treatment, the surgical approach, and the expected outcome.
Type I — Sliding Hiatus Hernia (Most Common)
This is by far the most common variety, accounting for up to 90% of all hiatus hernias. In a sliding hernia, the gastro-oesophageal junction (where the food pipe meets the stomach) slides up through the hiatus into the chest. The stomach itself moves up and down — hence the term 'sliding.' Most cases of chronic GERD (gastro-oesophageal reflux disease) are associated with this type.
Type II — Pure Paraesophageal Hernia
Here, the gastro-oesophageal junction stays below the diaphragm in its correct position, but a portion of the stomach rolls up beside the oesophagus into the chest. This type carries a higher risk of complications such as obstruction or strangulation, and often requires surgical correction even when symptoms appear mild.
Type III — Mixed Hernia
A combination of Types I and II, where both the gastro-oesophageal junction and a portion of the stomach are displaced into the chest. These hernias tend to be larger and more symptomatic.
Type IV — Complex Paraesophageal Hernia
The most advanced form. In addition to the stomach, other abdominal organs — such as the colon, spleen, or even part of the pancreas — may be displaced into the chest cavity. These are rare but represent a surgical emergency when complications develop.
Unlike abdominal wall hernias such as inguinal or umbilical hernias — covered under our hernia surgery in delhi service — a hiatus hernia involves the diaphragm and requires a completely different surgical approach.
Symptoms Of Hiatus Hernia
Ignoring persistent reflux can lead to strictures, Barrett’s oesophagus, or aspiration. Seek a specialist if you notice:
- Persistent heartburn: A burning sensation in the chest or throat, especially after meals or when lying down, that keeps coming back despite medication.
- Regurgitation: Sour or bitter liquid rising into the mouth without warning, particularly at night.
- Difficulty swallowing (dysphagia): Food getting stuck or a sensation of something in the throat.
- Chest pain or pressure: Often mistaken for heart-related symptoms; can be alarming and should always be evaluated.
Chest pain and bloating from hiatus hernia can closely mimic gallbladder disease — if you are unsure which is causing your symptoms, our team evaluates both; read about our gallbladder surgery service for comparison - Chronic cough or hoarseness: Acid reaching the vocal cords or airway causes persistent throat irritation, morning hoarseness, or a non-productive cough.
- Bloating and early satiety: Feeling uncomfortably full after small meals.
- Anaemia: In large paraesophageal hernias, repeated trauma to the stomach lining can cause slow bleeding, leading to iron-deficiency anaemia (Cameron lesions).
- Breathlessness: Large hernias can compress the lungs, causing breathing difficulties — particularly in elderly patients.
How We Diagnose a Hiatus Hernia
At Habilite Clinics, We believe in a thorough, evidence-based work-up before any treatment decision is made whether surgical or non-surgical. the following investigations are done before offering a customized treatment plan to our patients.
1. Upper GI Endoscopy
This is usually our first-line investigation. A thin, flexible camera is gently passed through the mouth to directly visualise the oesophagus, the gastro-oesophageal junction, and the stomach. Endoscopy allows us to:
- Confirm the presence and type of hernia
- Assess the degree of oesophagitis (inflammation from acid damage)
2. Barium Swallow X-Ray (Upper GI Series)
The patient drinks a barium-containing liquid that coats the digestive tract, making it visible on X-ray. This dynamic study is particularly valuable for mapping the anatomy of the hernia.
3. High-Resolution Oesophageal Manometry (HRM)
This test measures the pressures and movement patterns of the oesophagus. A thin catheter with multiple pressure sensors is placed through the nose into the oesophagus. HRM is essential for:
- Evaluating oesophageal motility — how well the food pipe propels food downward
- Assessing the function of the lower oesophageal sphincter (LES)
- Identifying achalasia or other motility disorders that would change our surgical approach
4. 24-Hour Ambulatory pH Monitoring
This is the gold-standard test for documenting acid reflux. A small probe or wireless capsule placed in the lower oesophagus measures acid levels continuously over 24 to 48 hours — including during meals, sleep, and daily activity. This tells us:
- Whether reflux is truly happening (and how frequently)
- Whether symptoms correlate with acid events
When Is Hiatus Hernia Surgery Necessary?
We never advice hiatus hernia surgery for every patients. For small, asymptomatic sliding hernias in older patients with no complications, conservative management may be entirely appropriate.
However, surgery is recommended in the following situations:
- Failed medical therapy: Symptoms persist despite optimised PPI therapy for 3–6 months, or the patient is unwilling to remain on lifelong medication.
- Large or paraesophageal hernia (Types II, III, IV): These carry a significant risk of volvulus (twisting), strangulation, or acute obstruction — even when asymptomatic. Most guidelines recommend elective surgical repair for symptomatic paraesophageal hernias to prevent life-threatening emergencies.
- Complications of GERD: Barrett's oesophagus, peptic stricture, severe oesophagitis (Grade C or D), or recurrent aspiration pneumonia.
- Anaemia from Cameron lesions: Recurrent bleeding from the herniated stomach segment causing iron deficiency.
- Respiratory symptoms: Documented aspiration, chronic cough, or exacerbation of asthma linked to reflux.
- Medication side effects or preferences: Patients who cannot tolerate or do not wish to continue long-term PPI therapy.
- Young, fit patients with established GERD: Surgery often provides a definitive, long-term cure versus decades of daily medication.
Lifestyle Modifications
- Lose excess weight, quit smoking, and avoid tight clothing around the abdomen.
- Eat small, frequent meals; stay upright for two hours after eating; avoid late-night dinners.
- Elevate the head end of the bed, skip high-fat or spicy meals, and limit caffeine or alcohol.
If you are not yet ready for surgery, our supervised medical weight-loss programme can lower intra-abdominal pressure and ease reflux through structured weight reduction.
Medicines for GERD & Hiatus Hernia
Medicines provide relief but cannot correct the diaphragm defect. Plans are titrated to avoid chronic dependence.
- Proton pump inhibitors and H2 blockers reduce acid production but do not cure the hernia.
- Antacids or alginate-based liquids provide quick relief from breakthrough symptoms.
- Medication plans are reviewed regularly to limit side-effects and nutrient deficiencies.
Laparoscopic Hiatus Hernia Surgery in Delhi
Laparoscopic (keyhole) surgery is the international gold standard for hiatus hernia repair for the past two decades. We perform the surgery through 4 to 5 small incisions of 5–10 mm. We introduce a high-definition camera and precision instruments. The herniated stomach is gently reduced back below the diaphragm, the hiatal defect is closed with sutures (cruroplasty), and the appropriate fundoplication is fashioned.
The major benefits for the laparoscopic approach are:
- Significantly less pain and blood loss
- Faster recovery — most patients return home within 24–48 hours
- Lower risk of wound complications and incisional hernia
- Quicker return to normal diet and activity
- Equivalent and in many studies’ superior long-term outcomes
Robotic Hiatus Hernia Repair in Delhi
We offer robot-assisted hiatus hernia surgery for selected patients, particularly those with large, complex, or recurrent hernias, or where the anatomy demands extreme precision. The major benefits offered by the robotic system are:
- Three-dimensional, magnified high-definition vision of the surgical field
- Wristed instruments that can reach angles impossible with conventional laparoscopy
- Superior dexterity for delicate crural suturing in a deep, narrow surgical space
- Tremor filtration for precise, controlled movements
Robotic surgery does not mean the robot operates independently — I control every movement at a surgical console. What it means for you is a more precise repair, with the same minimally invasive benefits and, in complex cases, potentially better outcomes. For a deeper comparison of both approaches, our guide on robotic versus laparoscopic surgery breaks down the trade-offs.
Laparoscopic vs Robotic Hiatus Hernia Comparison
| Feature | Laparoscopic | Robotic |
|---|---|---|
| Incisions | 4–5 small keyhole incisions | 4–5 small keyhole incisions |
| Hospital Stay | 1–2 days | 1–2 days |
| Pain level | Low to moderate | Low to moderate |
| Precision for Complex Cases | Excellent | Superior (3D vision + wristed instruments) |
| Recovery to Normal Activity | 4–6 weeks | 4–6 weeks |
| Best for | Most hiatus hernia repairs | Large/recurrent/complex hernias |
| Surgeon Control | Direct laparoscopic control | Robotic console — surgeon controls all movements |
Types of Fundoplication
One of the most important decisions in hiatus hernia surgery is choosing the correct type of fundoplication. Dr.Kapil Agrawal, one of the best hiatus hernia specialist, performs complete range of fundoplication with excellent outcomes. Our choice of fundoplication is guided by your symptoms, your oesophageal manometry findings, and the size of your hernia.
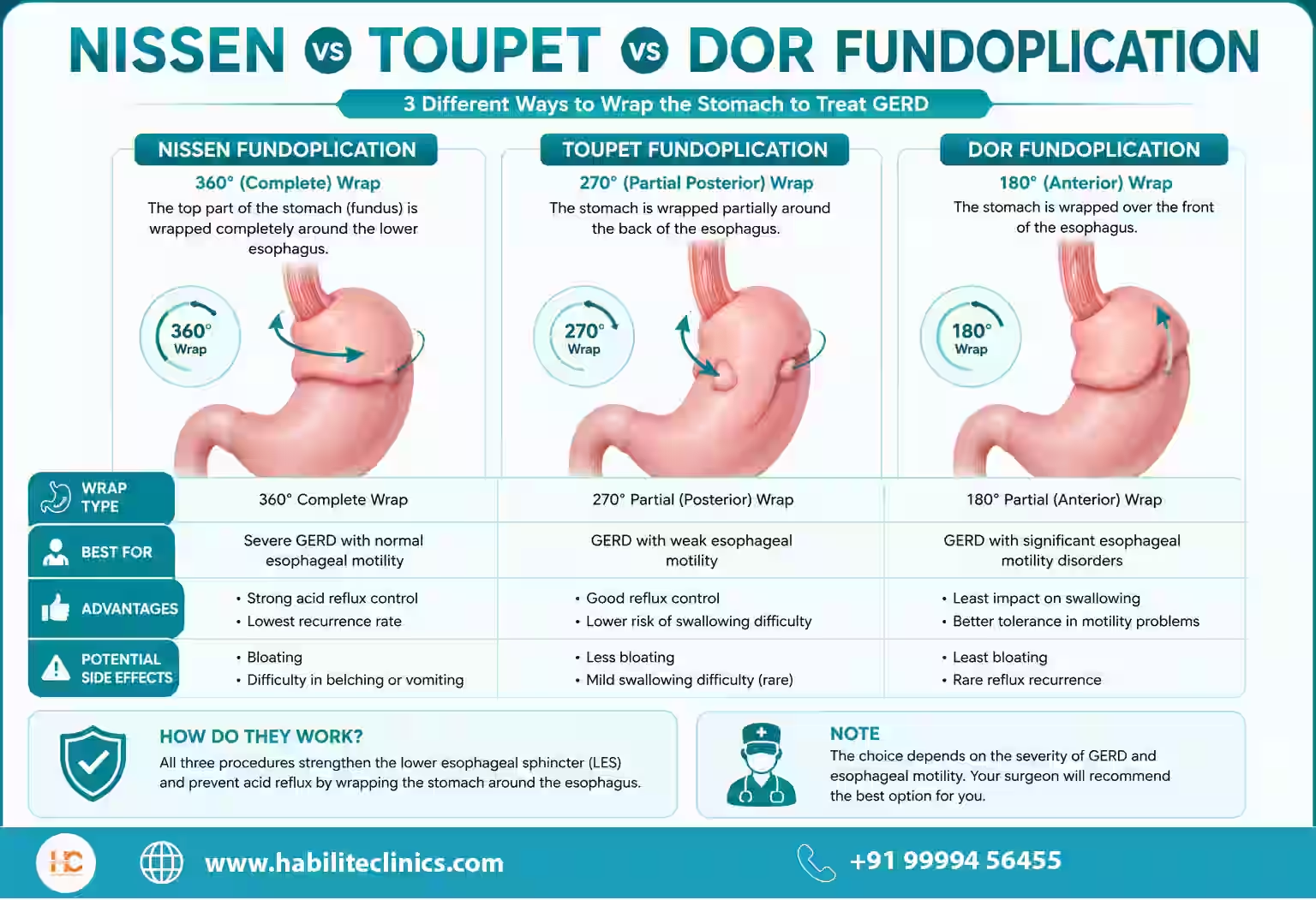
Nissen Fundoplication
This is the most commonly performed anti-reflux procedure worldwide and has the longest track record. The fundus (upper part) of the stomach is wrapped fully around the lower oesophagus to create a 360-degree sleeve. This provides the strongest anti-reflux barrier.
We offer Nissen fundoplication in patients with normal oesophageal motility and documented significant acid reflux. Offers excellent long-term reflux control.
Consideration: In patients with weak or uncoordinated oesophageal peristalsis, the tight wrap can cause difficulty swallowing (dysphagia). This is why manometry is essential before choosing Nissen.
Toupet Fundoplication
In Toupet fundoplication, the stomach is wrapped only around the back portion of the oesophagus — covering approximately 270 degrees. This partial posterior wrap provides effective reflux control while preserving the ability to swallow comfortably.
Toupet fundoplication is best for patients with borderline or impaired oesophageal motility where a total wrap carries a risk of post-operative dysphagia.
Toupet tends to have fewer obstructive side effects and better quality of life scores, particularly for paraesophageal hernia repair.
Dor Fundoplication
The stomach is wrapped around only the front of the lower oesophagus. This is the most conservative wrap and creates the least resistance.
We perform Dor fundoplication in patients with significant oesophageal dysmotility or achalasia who require concurrent myotomy (Heller's procedure). We also use this fundoplication in select situations where posterior dissection carries technical risk.
| Fundoplication Type | Wrap Degree | Best For |
|---|---|---|
| Nissen (Total) | 360° posterior | Normal motility, severe reflux, sliding hernia |
| Toupet (Partial Posterior) | 270° posterior | Borderline motility, paraesophageal hernia, dysphagia risk |
| Dor (Anterior) | 180° anterior | Impaired motility, achalasia with myotomy |
Mesh in Hiatus Hernia Repair — When and Why
We use mesh in hiatus hernia repair only for larger hiatal defects greater than 5 cm where simple suture closure of the hiatal gap can increase the risk of recurrence.
In such cases, we reinforce the crural closure with a prosthetic mesh. The decision to use mesh, and the choice of mesh, is made based on the size of the defect and the technical findings at the time of surgery.
Hiatus Hernia with Obesity: The Combined Bariatric-Reflux Approach
Obesity is a major contributing factor to hiatus hernia and GERD. Elevated intra-abdominal pressure from excess weight forces the stomach upward, weakens the hiatal mechanism, and dramatically worsens reflux.
At Habilite Clinics, we offer a simultaneous hiatus hernia repair and bariatric procedure — typically a sleeve gastrectomy or Roux-en-Y gastric bypass For patients whose reflux is driven primarily by excess weight, our dedicated bariatric surgery programme assesses whether weight-loss surgery alone — or combined with hiatal repair in a single session — offers the most durable result.
This avoids two separate operations, addresses the root cause of reflux, and produces dramatic, sustained improvements in both weight and reflux symptoms.
Patients who have had previous abdominal surgery and are also managing reflux should be aware that combined pressure from both conditions can increase risk of incisional hernia at prior scar sites — we assess for this at consultation.
Cost of Hiatus Hernia Surgery in Delhi
The cost of hiatus hernia surgery in Delhi varies depending on the type of hernia, the surgical approach used, the hospital facility, and whether any additional components such as mesh reinforcement are required. Below is an honest, transparent overview of what you can expect at Habilite Clinics and by our team
Approximate Cost of Hiatus Hernia Surgery in Delhi
| Surgery Type | Approximate Cost Range (Delhi) | Hospital Stay | What's Typically Included |
|---|---|---|---|
| Laparoscopic Hiatus Hernia Repair (Sliding / Small Hernia) | ₹75,000 – ₹1,20,000 | 1–2 days | Surgeon fee, OT charges, anaesthesia, consumables, 1–2 day stay |
| Laparoscopic Repair with Fundoplication (Nissen / Toupet / Dor) | ₹1,00,000 – ₹1,60,000 | 1–2 days | All above + fundoplication wrap, post-op diet counselling |
| Laparoscopic Repair with Mesh (Large / Paraesophageal Hernia) | ₹1,20,000 – ₹1,80,000 | 2–3 days | All above + prosthetic mesh reinforcement |
| Robotic Hiatus Hernia Repair (Complex / Recurrent Cases) | ₹1,80,000 – ₹2,80,000 | 2–3 days | Robotic platform charges + all components above |
| Combined Bariatric + Hiatus Hernia Repair (Obesity + GERD) | ₹2,20,000 – ₹3,50,000 | 2–4 days | Combined procedure in single session — avoids two separate surgeries At Habilite Clinics, we offer simultaneous hiatus hernia repair and our bariatric surgery in Delhi — sleeve gastrectomy or gastric bypass — in a single operative session. |
GERD & Hiatus Hernia Surgery Cost in Delhi
Get accurate cost estimate for your treatment
Diet After Hiatus Hernia Surgery
What you eat in the weeks following hiatus hernia surgery is not a minor detail but core part of your recovery.
The fundoplication wrap causes temporary swelling at the lower end of the food pipe, making the passage narrower than usual. Eating the wrong foods too early can cause food to get stuck, put pressure on the repair, or cause significant discomfort.
For a complete week-by-week guide — including an Indian meal plan, foods to avoid, and answers to the most common dietary questions after surgery — read our dedicated blog: Diet After Hiatus Hernia & GERD Surgery.
Recovery After Hiatus Hernia Surgery
Recovery from laparoscopic or robotic hiatus hernia surgery is, for most patients, considerably easier than they expected. The minimally invasive approach means no large wound to heal, less pain, and a much faster return to normal life than open surgery.
That said, the internal repair needs time to consolidate — and the dietary and activity guidance in the first 6 weeks is important to follow. Here is what to expect, stage by stage.
| Timeline | Recovery Milestone | Activity & Guidance |
|---|---|---|
| Day 1–2 | In hospital | Mobilise within hours of surgery. Start sipping clear liquids. Pain well-controlled with oral medication. |
| Day 2 | Discharge home | Most patients go home within 24–48 hours. Pain described as mild to moderate — like muscle soreness around the abdomen. |
| Week 1 | Completely mobile at home | Long, gentle walks encouraged. Avoid any lifting, straining, or bending. Continue clear liquid diet. No driving. |
Habilite Clinics' Free Post-operative Care
We provide comprehensive free post-operative care to ensure your smooth recovery and optimal results. Our dedicated team is committed to your well-being throughout your healing journey.
Comprehensive Care
Complete post-operative support and monitoring
Expert Guidance
24/7 access to our medical team
Dedicated Support
Personalized care coordinator for each patient
Regular Follow-ups
Scheduled check-ups to ensure optimal recovery
What's Included in Our Free Post-operative Care:
- ✓Regular follow-up consultations with Dr. Kapil Agrawal
- ✓24/7 emergency support and guidance
- ✓Nutritional counseling and diet plans
- ✓Wound care and dressing assistance
- ✓Medication management and adjustments
- ✓Progress monitoring and recovery assessment
Frequently Asked Questions
Everything you need to know about GERD and hiatus hernia symptoms, treatment choices, recovery timelines, and insurance assistance.
A hiatus hernia occurs when part of the stomach slides into the chest through the diaphragm. Medicines and lifestyle changes help small hernias, but symptomatic or paraesophageal ones need laparoscopic repair plus fundoplication.
Over 90% of patients report long-term reflux relief. The hiatal defect is repaired, the stomach is wrapped around the oesophagus, and recovery takes about a week with minimal restrictions.
Patients walk within hours, start liquids the same day, and are discharged within 24–36 hours. Desk work resumes in about a week with guided diet advancement.
Medicines suppress acid and reduce irritation but cannot repair the anatomical defect. Symptomatic or large hernias eventually need surgery.
Surgery is recommended if symptoms persist on medicines, complications such as aspiration or Barrett's develop, or imaging shows a large paraesophageal hernia.
Follow a liquid diet for 7–10 days, transition to semi-solids for another 10 days, chew thoroughly, and avoid fatty or acidic meals initially.
GERD (gastro-oesophageal reflux disease) is the symptom — the backflow of acid causing heartburn and regurgitation. A hiatus hernia is a structural cause — a physical displacement of the stomach — that makes GERD more likely and more severe. Many patients with GERD have an underlying hiatus hernia, though not all hiatus hernias cause GERD.
Yes — many small, sliding hiatus hernias can be effectively managed with lifestyle changes (weight loss, avoiding large meals, not lying down after eating, elevating the head of the bed) and acid-suppressing medication. Surgery is recommended when symptoms cannot be controlled medically, when the hernia is large or paraesophageal, or when complications develop.
Laparoscopic hiatus hernia repair offers durable, long-lasting results. However, no surgical repair carries a zero recurrence rate. Large hernias, particularly those requiring mesh reinforcement, have a higher recurrence risk than small sliding hernias. Maintaining a healthy weight after surgery significantly reduces the risk of recurrence.
Fundoplication is the wrapping of part of the stomach around the lower oesophagus to recreate the anti-reflux valve. For symptomatic hiatus hernias associated with GERD, fundoplication is performed alongside the hiatal repair. For purely mechanical hernias in patients without significant reflux (some Type II/III hernias), fundoplication may be omitted or modified based on manometry findings.
This decision should be based on your oesophageal manometry results. Patients with normal motility are good candidates for Nissen (360-degree). Those with borderline motility generally fare better with Toupet (270-degree). Patients with achalasia or severe dysmotility need Dor (180-degree) or no fundoplication at all. I discuss this in detail with every patient before surgery.
Most patients return home within 24–48 hours. You will follow a liquid-to-soft diet for 4–6 weeks. Most people return to desk work within 7–10 days and are fully active within 4–6 weeks.
For most straightforward hiatus hernias, standard laparoscopic surgery provides excellent results. Robotic surgery offers additional precision and dexterity that is particularly valuable in large, complex, or recurrent hernias where the anatomy is challenging. I recommend robotic surgery when the clinical situation genuinely warrants it — not as a routine upgrade.
The cost of hiatus hernia repair in Delhi varies depending on the hospital, the complexity of the hernia, whether standard laparoscopic or robotic surgery is used, and the length of hospital stay. At Habilite Clinics, we offer transparent cost counselling during your consultation and assist with cashless insurance processing wherever applicable. Please contact our team for an individualised estimate.
Yes. Large hiatus hernias can press against the heart and pericardium, causing palpitations, an irregular heartbeat, or a rapid heart rate (tachycardia). This is an important — and often unrecognised — symptom that always warrants cardiac evaluation followed by assessment for a large hiatus hernia.
Laparoscopic hiatus hernia repair can be safely performed in appropriately selected elderly patients. The minimally invasive approach significantly reduces the physiological stress of surgery compared to open repair. I assess each patient is fitness individually, taking into account co-existing medical conditions, anaesthetic risk, and the natural history of the hernia.
Related GERD & Hiatus Hernia Blogs
Expert insights, tips, and guides about gerd & hiatus hernia
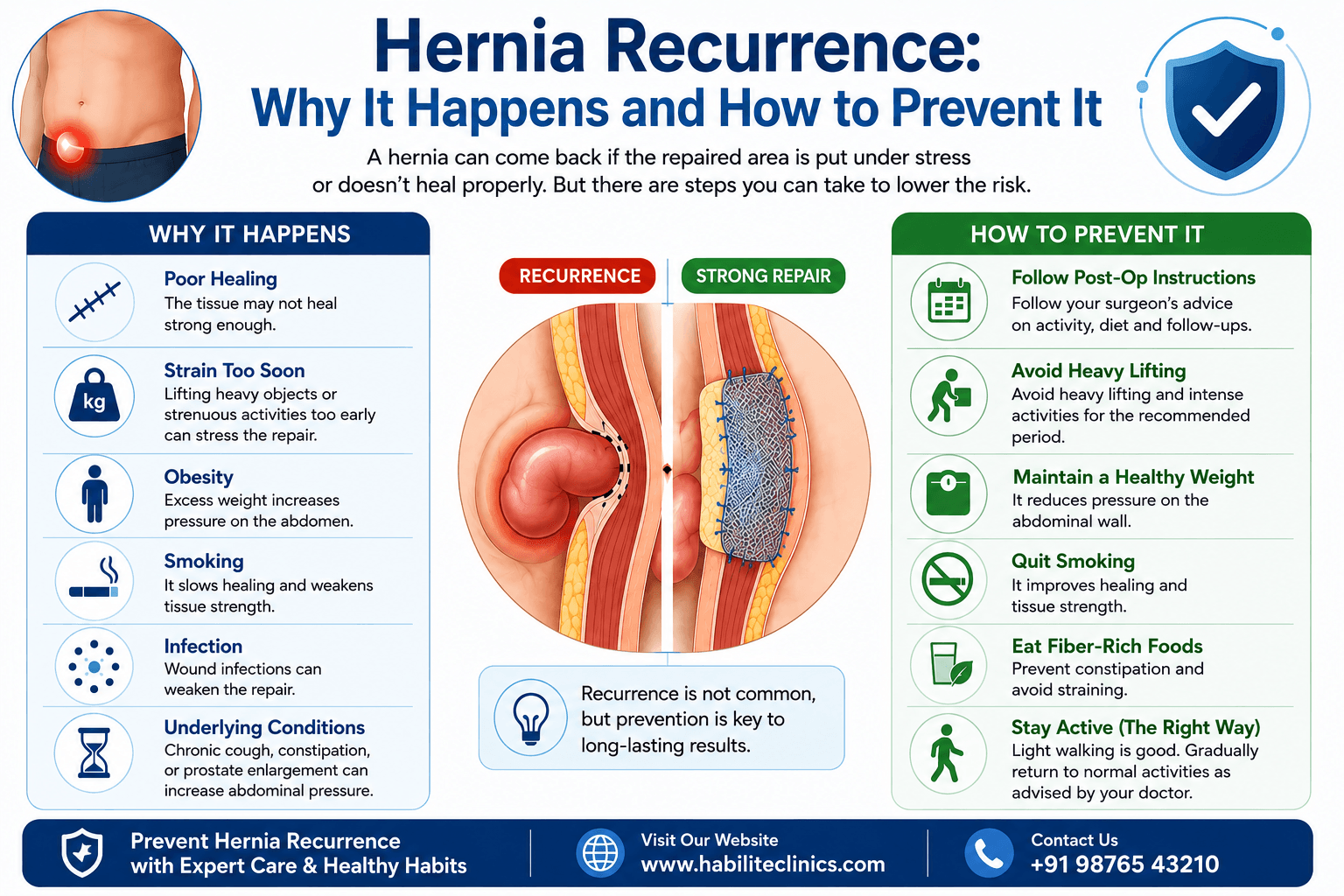
Hernia Recurrence: Why It Happens and How to Prevent It
You have been through a hernia surgery. The recovery was uncomfortable. You followed the doctor's advice. And now, months or even years later, you feel a familiar lump or twinge in exactly the same spot. A wave of worry washes over you.
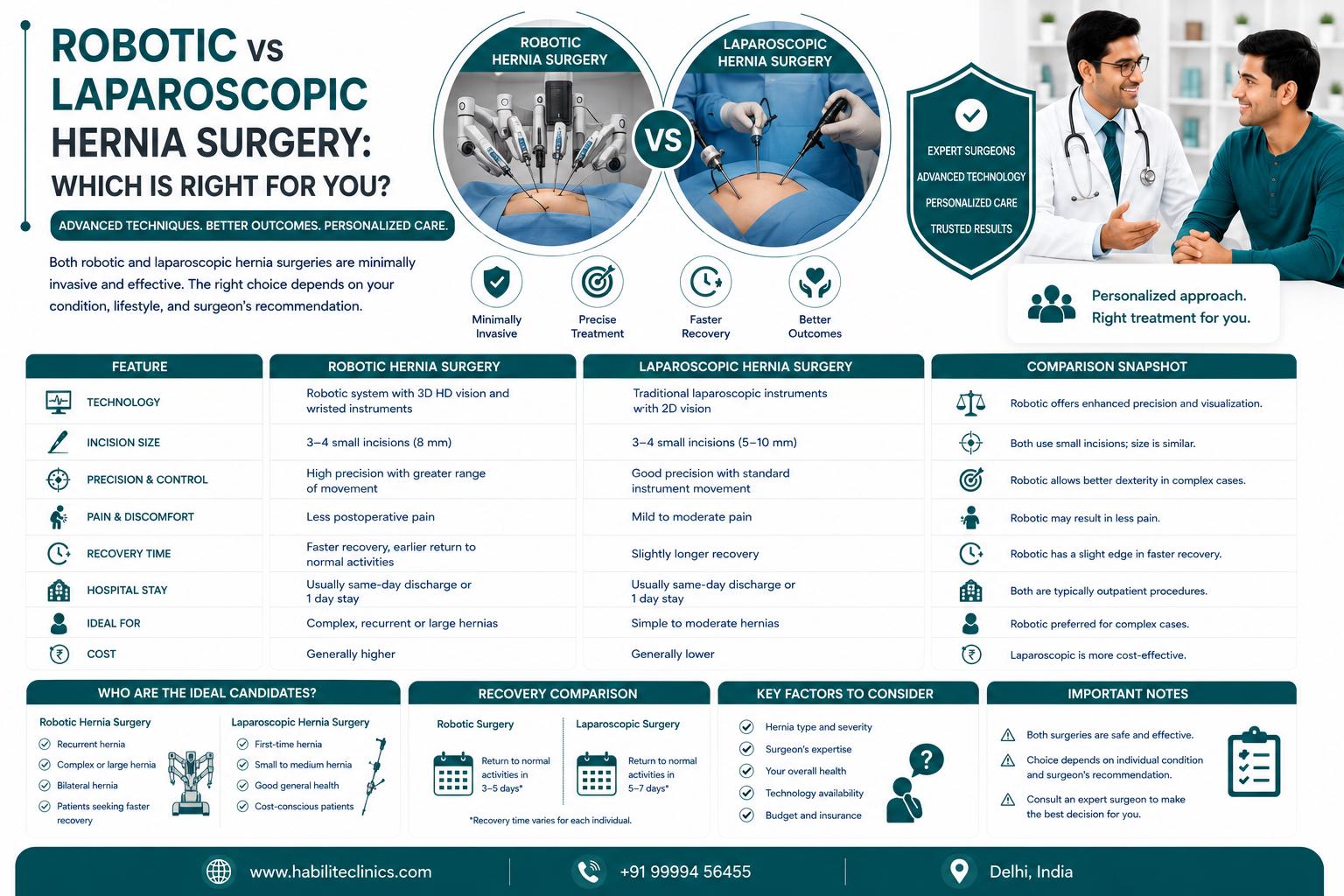
Robotic vs Laparoscopic Hernia Surgery: Which Is Right for You?
Both robotic and laparoscopic hernia surgeries are minimally invasive options with smaller cuts, less pain, and faster recovery than traditional open surgery. ✓ Robotic hernia surgery offers 3D high-definition vision, greater precision with 540-degree instrument rotation, and tremor filtration for complex cases. ✓ Laparoscopic surgery is more widely available, more affordable (₹40,000-50,000 less expensive), and equally effective for most standard hernias. ✓ Dr. Kapil Agrawal and our team at Habilite Clinics offer both techniques with 23+ years of surgical experience. ✓ The choice between robotic and laparoscopic depends on hernia type, complexity, prior surgeries, patient health, and cost considerations—not all patients need robotic surgery. ✓ Both procedures have been covered by health insurance in India since 2019 under IRDAI guidelines, making advanced minimally invasive surgery accessible to more patients.
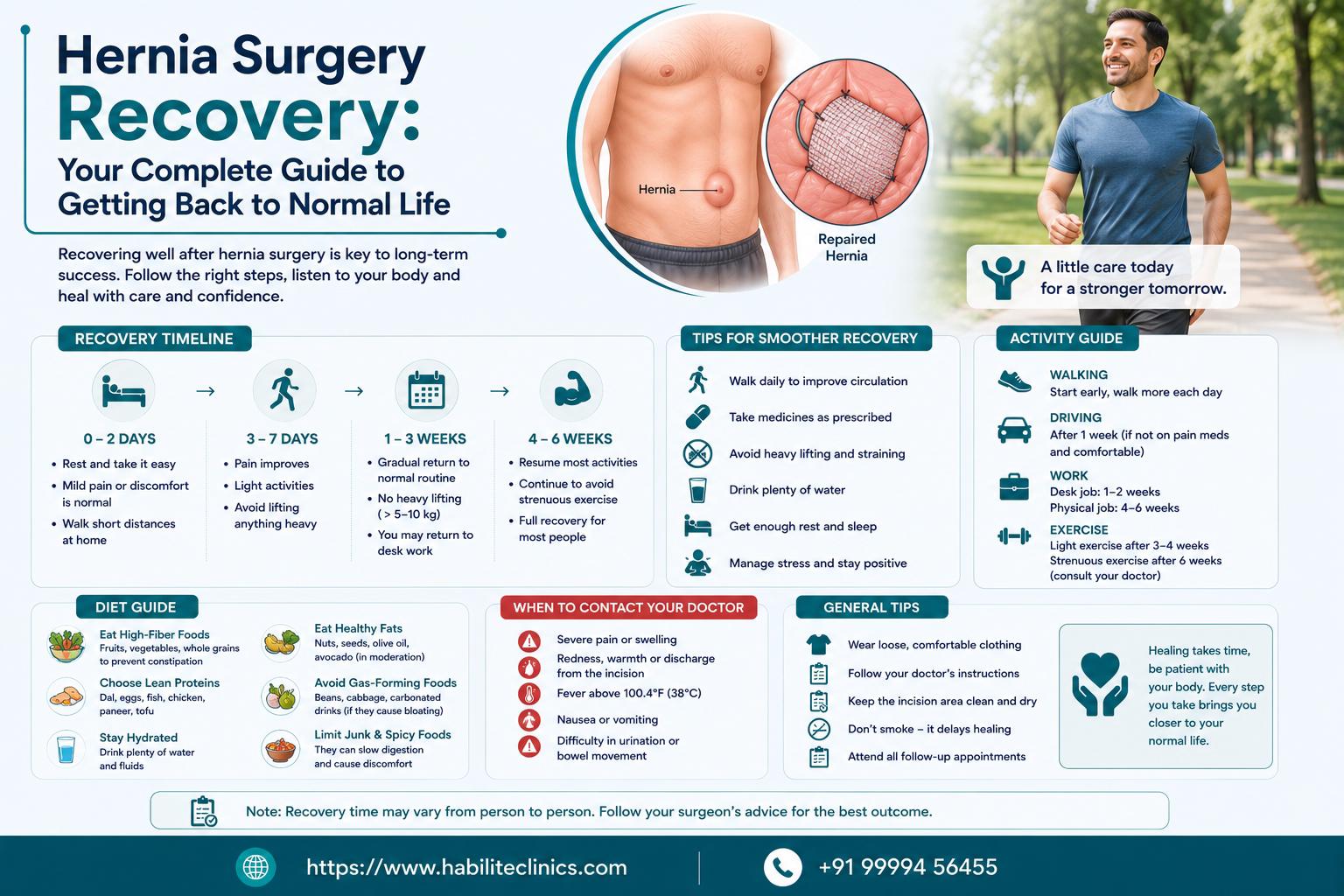
Hernia Surgery Recovery: Your Complete Guide to Getting Back to Normal Life
Recovery varies by surgery type: Laparoscopic hernia surgery recovery takes 1-2 weeks for light activities, while open surgery may need 4-6 weeks Early movement is essential: Walking within hours of surgery prevents blood clots and speeds healing. Complete bed rest is outdated and harmful You can eat normal food, use Indian toilets, and don't need months of rest after modern hernia surgery A protein-rich diet accelerates healing: Focus on eggs, dal, chicken, and fish to rebuild muscle strength after surgery Warning signs need immediate attention: Sudden severe pain, fever above 101°F, or inability to pass gas requires urgent medical care Return to work depends on your job: Desk jobs allow return in 1-2 weeks; manual labor jobs need 4-6 weeks recovery