
Femoral Hernia Surgery in Delhi — by Dr. Kapil Agrawal
If you have noticed a small, tender lump high up on your inner thigh or groin crease — one that may come and go, may feel firmer than the surrounding tissue, and may be dismissed as a 'pulled muscle' or a 'swollen lymph node' — please read this page carefully. You may be dealing with a femoral hernia.
Femoral hernia is one of the most under-diagnosed and over-complicated hernias we treat at Habilite Clinics. It is uncommon — accounting for only about 3% of all groin hernias — but it has a disproportionately high risk of becoming a surgical emergency. Roughly 1 in 3 femoral hernias presents for the first time as a strangulated hernia, where the trapped tissue loses its blood supply and surgery cannot wait.
I am Dr. Kapil Agrawal, Senior Consultant Surgeon at Apollo Hospitals, Delhi NCR. Over the past 23 years and across 7,000+ hernia repairs, I have developed a special focus on femoral hernia surgery in Delhi — particularly for women, who account for the overwhelming majority of these cases. If you are looking for the best hernia surgeon in Delhi, you are in the right place.
Book Consultation
Schedule a consultation for Femoral Hernia Surgery with Dr. Kapil Agrawal
What Is a Femoral Hernia?
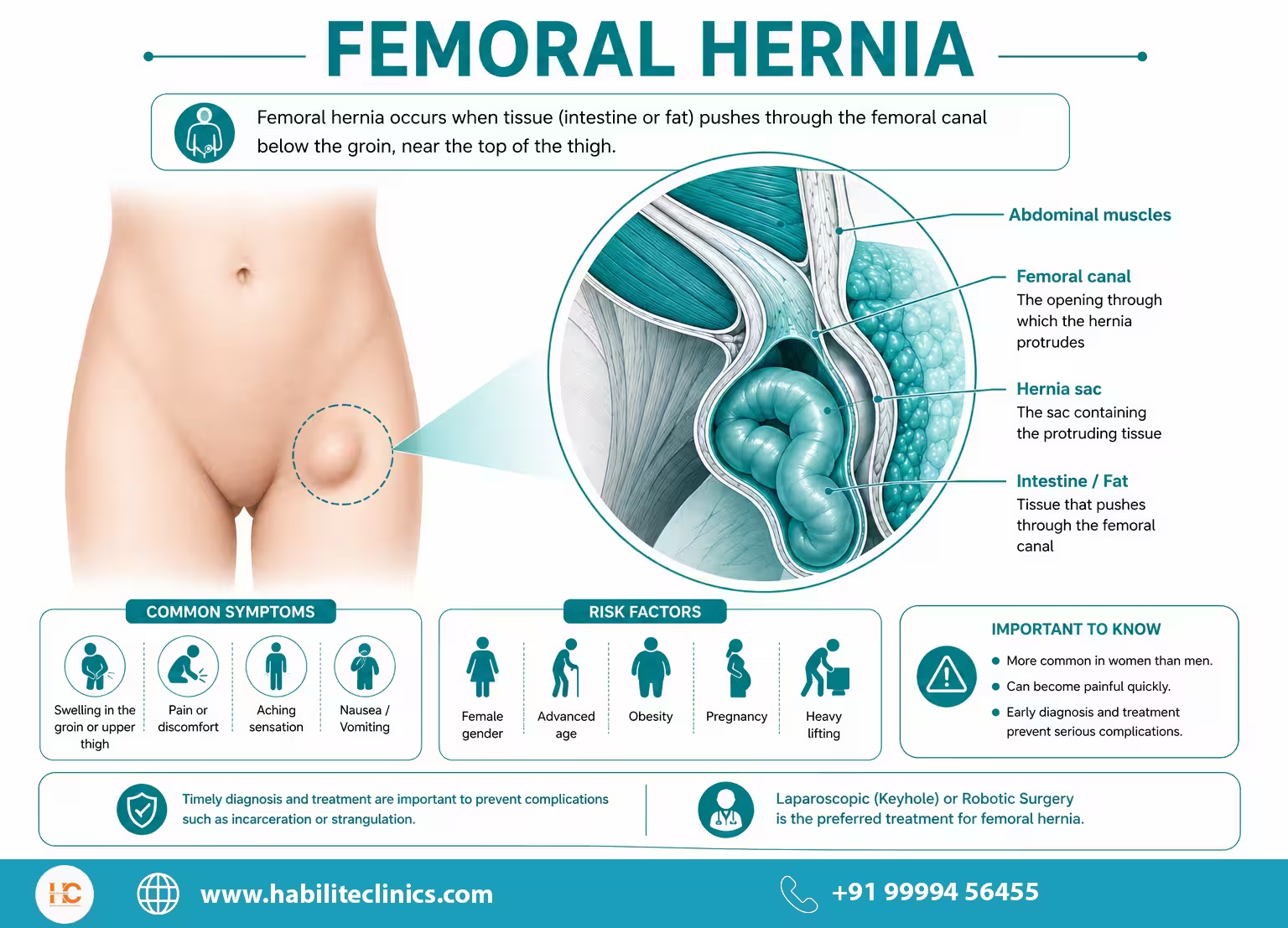
A femoral hernia occurs when a portion of your intestine, fat, or abdominal tissue pushes through a small, naturally weak space called the femoral canal — a narrow tunnel that lies in your upper thigh, just below the groin crease. This canal is normally a passageway for major blood vessels (the femoral artery and vein) traveling from your abdomen down into your leg. When the surrounding connective tissue weakens, abdominal contents can squeeze into this tight space and form a femoral hernia.
If you are new to the condition, it helps to first understand what a hernia is, its causes, symptoms, and treatment options.
You will usually first notice a femoral hernia as:
- A small, firm bulge high up on the inner thigh, just below the groin crease
- A tender, sometimes painful lump that becomes more obvious when you stand, walk, or strain
- A dragging or pinching sensation in the upper thigh, especially by the end of the day
- Discomfort that worsens with prolonged standing or after household work
- In some cases, no symptoms at all — until the day it suddenly becomes very painful
Here is what makes a femoral hernia different from any other hernia I treat: the femoral canal is extremely narrow and rigid, surrounded by tough ligaments on three sides. Once tissue squeezes into this small space, it can get trapped very quickly — and that is exactly why femoral hernias have the highest emergency rate of all abdominal wall hernias.
Why Femoral Hernia Is Far More Common in Women
Of every 10 femoral hernia patients I see at Habilite Clinics, roughly 7 to 8 are women. The reason is anatomical, and once you understand it, the risk factors will make complete sense to you.
The female pelvis is wider than the male pelvis to accommodate childbirth. As a result, the femoral canal in women is naturally larger and more vulnerable to herniation. Add to this the lifetime hormonal, postural, and pressure-related changes a woman's body goes through, and you have a clear picture of who is most at risk.
You are at higher risk of developing a femoral hernia if:
- You are a woman between the ages of 40 and 70 — this is the peak demographic in our OPD
- You have had multiple pregnancies, particularly with large babies or prolonged labour
- You are in or past menopause — declining estrogen weakens connective tissue
- You are overweight or have significant abdominal obesity
- You have chronic constipation and strain regularly during bowel movements
- You have a chronic cough from smoking, asthma, or respiratory conditions
- You have had a previous abdominal or pelvic surgery (hysterectomy, C-section, ovarian cyst removal)
- You do heavy lifting at home or at work — including elder care or domestic work
- You have a previous history of inguinal hernia repair on the same side
Several of these risk factors are modifiable — I cover them in our guide on how to prevent a hernia. If two or more of these apply to you and you have noticed a tender bulge or vague groin pain, please do not wait. A 15-minute clinical examination is all I need.
Femoral Hernia vs. Inguinal Hernia — Why It's So Often Missed
This is one of the most important sections on this page. Both femoral and inguinal hernias produce a bulge in the same general region of the body — and to an untrained eye, even an experienced general practitioner's, they can look identical. However, they exit through completely different anatomical openings and require subtly different surgical approaches.
| Feature | Inguinal Hernia | Femoral Hernia |
|---|---|---|
| Location of bulge | Above the groin crease (inguinal ligament) | Below the groin crease, on upper inner thigh |
| Common in | Men (90% of cases) | Women (70–80% of cases) |
| Size | Usually larger, can extend into scrotum or labia | Usually smaller, often pea-to-walnut sized |
| Pain pattern | Pulling, dragging, often mild | Tender, pinching, often disproportionate to size |
| Strangulation risk | 1–3% per year | 15–20% lifetime — highest of any hernia |
| Reducibility | Often easy to push back in | Often difficult or impossible to reduce |
| Best surgery | TEP / TAPP / eTEP / Lichtenstein | Laparoscopic TAPP / Robotic / McVay |
Why does this matter to you? Because a femoral hernia mistakenly treated as an inguinal hernia can be missed entirely on the operating table if the surgeon does not specifically look for it. This is one of the most common reasons we see "recurrent" hernias in women referred to us — the original surgery missed the femoral defect alongside the inguinal one.
When you come to me, I specifically examine for both. If you are unsure whether your symptoms warrant a surgical opinion yet, this guide on the signs you need hernia surgery will help.
If you are unsure which type of hernia you have, please also read our page on inguinal hernia surgery in Delhi.
How I Diagnose Your Femoral Hernia
Femoral hernia diagnosis can be tricky, and that is exactly why specialist hands matter here. In my consultation, I will:
- Take a careful history — your symptoms, their pattern, your obstetric history, your weight changes, and any previous groin surgery
- Examine you standing and lying down — femoral hernias often disappear when you lie flat and become obvious only when you stand and cough
- Differentiate from common mimics — these include lipoma, enlarged inguinal lymph node, saphena varix, psoas abscess, and femoral artery aneurysm
When clinical examination is uncertain — which happens more often in femoral than in inguinal hernias — I rely on:
- High-resolution groin ultrasound (USG) — the most accurate, painless, and immediate diagnostic test
- Dynamic MRI groin — useful when the bulge is intermittent or when sportsman's hernia is also suspected
- CT scan with Valsalva manoeuvre — for large, recurrent, or emergency presentations where I need to map vascular anatomy precisely
Confused about your ultrasound report? You can share your ultrasound report on WhatsApp and our team will explain every finding to you in plain English.
Why You Cannot Afford to Delay Femoral Hernia Surgery
I want to be very direct with you here. I tell every patient with an inguinal hernia that surgery should not be delayed — but for a femoral hernia, the urgency is genuinely greater. Here is why.
The femoral canal is bordered by four rigid structures: the inguinal ligament above, the pectineal (Cooper's) ligament behind, the lacunar ligament medially, and the femoral vein laterally. Unlike the inguinal canal, the femoral canal cannot stretch to accommodate the herniated tissue. This means:
- Strangulation can occur within hours, not days or weeks. Roughly 1 in 3 femoral hernia patients first present to a hospital with a strangulated hernia
- The lifetime risk of strangulation in an untreated femoral hernia is 15–20% — far higher than the 1–3% lifetime risk in an inguinal hernia
- Strangulated tissue can die in 4–6 hours, which may require removal of a portion of the bowel and a much bigger emergency operation
- Emergency surgery has higher complication rates and longer recovery than planned, elective surgery
In short — once a femoral hernia is diagnosed, planned, elective laparoscopic repair is almost always the right answer, regardless of whether the hernia is currently causing major symptoms. Watchful waiting is not a safe strategy for femoral hernia.
To understand the bigger picture, read our blog: Is it safe to delay a hernia surgery?.
Modern Treatment Options for Femoral Hernia at Habilite Clinics
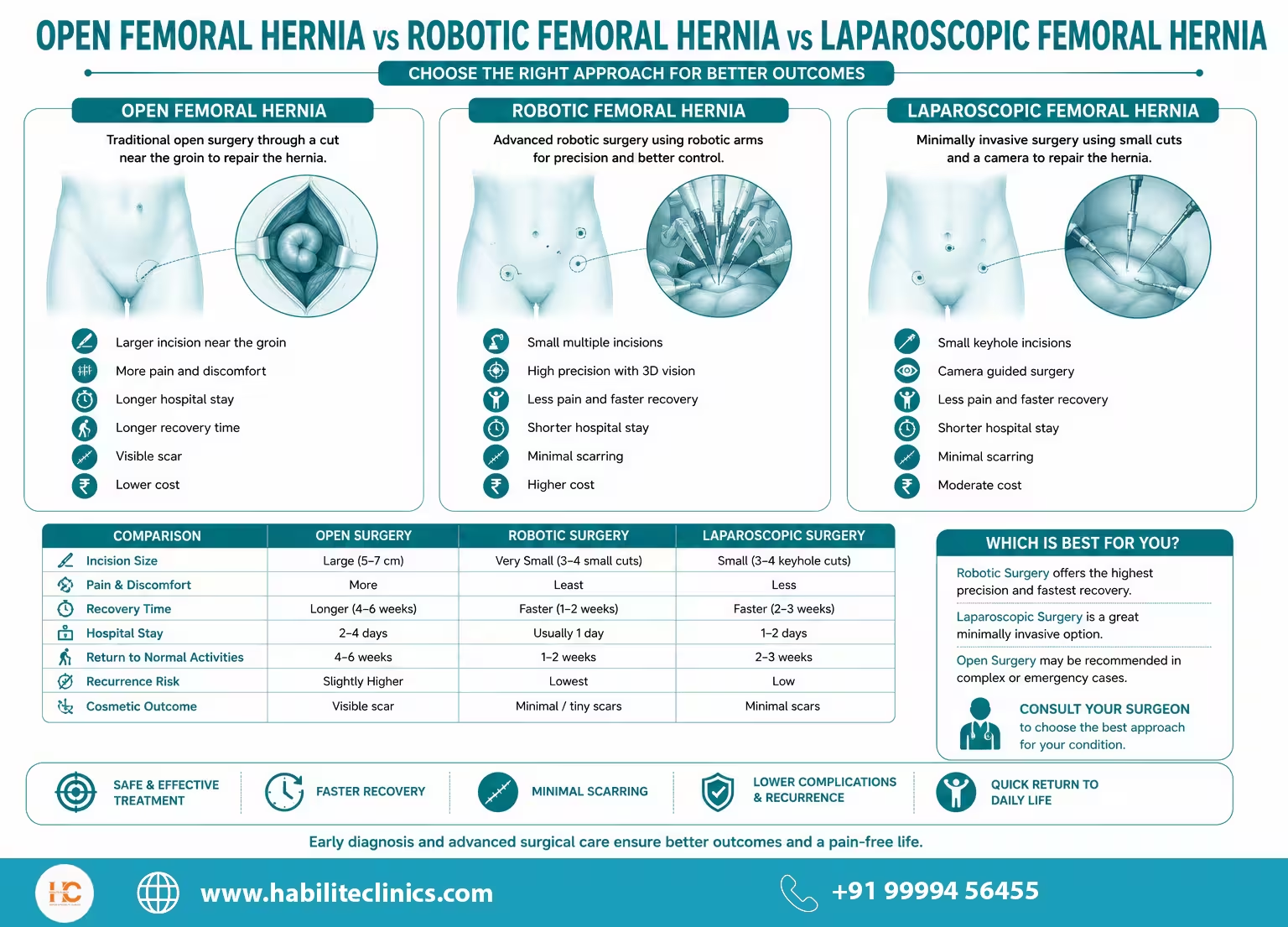
Because the femoral canal is anatomically more challenging than the inguinal canal, surgical approach selection matters. In my practice, I offer all three modern options — laparoscopic, robotic, and open — and choose based on your hernia size, body type, urgency, and overall health.
1. Laparoscopic Femoral Hernia Repair (Keyhole Surgery)
This is my preferred approach for the majority of femoral hernia patients, and here is why: laparoscopic surgery gives me a clear, magnified view of the entire myopectineal orifice — the deep groin region where both inguinal and femoral hernias originate. From this view, I can see and reinforce the femoral defect with a precisely placed mesh, while also checking and reinforcing the inguinal floor on the same side.
The benefits for you:
- 3 tiny incisions of 5–10 mm near the navel
- Significantly less post-operative pain than open repair
- Same-day or 24-hour discharge for most patients
- Return to desk work and household activity in 7–10 days
- Almost zero visible scarring once healed
- Both groins repaired simultaneously if you have a bilateral hernia
TAPP (Trans-Abdominal Pre-Peritoneal) Repair
This is my most common technique for femoral hernia. I enter the abdominal cavity, lift a flap of peritoneum, gently reduce the herniated tissue from the femoral canal, place a wide mesh covering the entire myopectineal orifice (which addresses both femoral and inguinal weak points), and close the peritoneal flap. TAPP is particularly useful in incarcerated and emergency femoral hernias because it allows me to inspect the bowel from inside.
TEP (Totally Extra-Peritoneal) Repair
TEP is performed entirely outside the inner lining of the abdomen, with no entry into the abdominal cavity. I prefer TEP in slim patients with smaller, easily reducible femoral hernias and no previous lower abdominal surgery.
2. Robotic Femoral Hernia Surgery
Robotic-assisted femoral hernia repair takes the laparoscopic approach to its highest level of precision. Through the same small incisions, I control wristed instruments with a range of motion that exceeds the human hand, while viewing your groin anatomy in magnified 3D high-definition.
My detailed comparison of robotic vs laparoscopic hernia surgery explains when each approach makes a real difference.
I specifically recommend robotic femoral hernia repair for:
- Recurrent femoral hernias after a previous open or laparoscopic repair
- Femoral hernias with previous lower abdominal surgery (hysterectomy, C-section, prostate, bladder)
- Bilateral or combined inguinal-femoral hernias where multiple defects need precise mesh placement
- Obese patients where laparoscopic visualization is more challenging
Your recovery is identical to standard laparoscopic repair — the precision is on the operating table, not in the scars or the timeline.
3. Open Femoral Hernia Repair
Open surgery remains the right choice in specific situations — and I am clear with my patients about when. I use open femoral hernia repair when:
- You are presenting as an emergency with strangulated bowel that needs to be inspected and possibly removed
- You are unfit for general anaesthesia (severe heart or lung disease)
- You have had multiple previous laparoscopic repairs that have failed
- The hernia is very large with significant local scarring
McVay (Cooper's Ligament) Repair
This is the classical open femoral hernia repair. Through a small groin incision, I close the femoral canal by suturing the conjoined tendon directly to Cooper's (pectineal) ligament, blocking the femoral defect. A small piece of mesh may be added for reinforcement.
Plug-and-Patch / Lichtenstein Modification
For selected open repairs, a small mesh plug is placed into the femoral defect, with a flat mesh patch reinforcing the surrounding floor. Excellent results in elective non-strangulated cases.
Tissue Repair (No Mesh)
In strangulated emergency cases where bowel resection has been performed and there is contamination, mesh is contraindicated. In such patients, I perform a tissue-only repair (typically McVay) and plan a future definitive mesh repair if needed.
Mesh Selection for Femoral Hernia Repair
In modern, elective femoral hernia surgery, mesh is the global gold standard. To understand how surgical mesh works, the materials I use, and what they cost, read our guide on hernia mesh: types, advantages, and cost. A correctly placed mesh reduces recurrence rates from 10–15% (without mesh) to under 2% (with mesh) — a significant improvement, particularly in women with pre-existing connective tissue weakness.
In my practice, I use only internationally validated, USFDA-approved meshes, and I select based on:
- Hernia size and the size of the myopectineal orifice
- Whether I am repairing femoral alone or femoral plus inguinal in the same operation
- Your body weight and BMI
- Whether the surgery is elective or emergency (mesh is avoided in contaminated emergency cases)
- Whether the mesh will be intra-peritoneal or pre-peritoneal
You will always know exactly which mesh I am placing in you and why. We do not hide mesh details inside the hospital bill.
Femoral Hernia Surgery — Day of Surgery, Step by Step
You will arrive at the hospital in the morning, fasting since midnight. Here is what your day looks like:
- Admission and pre-op (45 minutes): Vitals, IV line, anaesthesia consultation, OT team briefing
- Anaesthesia (10 minutes): General anaesthesia for laparoscopic and robotic; spinal or local for selected open repairs
- Surgery (45–75 minutes): Time depends on hernia size, side, technique, and whether bowel inspection or resection is needed
- Recovery (1–2 hours): You wake up in recovery, comfortable and oriented
- Mobilisation and discharge: Most non-insurance patients walk out the same day. Insurance/cashless cases are discharged within 24 hours
You go home with a printed recovery blueprint, your medication list, my direct contact details, and a personal care coordinator who will WhatsApp you every day for the first week.
For a complete preparation guide, read: How to prepare for a hernia surgery.
Recovery Timeline After Femoral Hernia Surgery
| Time After Surgery | What You Can Do |
|---|---|
| 2 hours | Sit up, sip water, pass urine, walk to the bathroom |
| 24 hours | Discharge, light home meals, short walks at home |
| 48–72 hours | Resume normal home diet, light activity, shower |
| Day 5–7 | Resume kitchen work, drive a car, return to desk job |
| Week 2 | Brisk walking, household chores, light shopping |
| Week 3–4 | Stationary cycling, treadmill, light yoga |
| Week 6 | Heavy lifting, gym, dancing, and full activity clearance |
These are guidelines — your personal timeline depends on your hernia, your overall fitness, and the technique used. I review every patient at 1 week, 1 month, and 3 months after surgery, and these consultations are complimentary for life.
Femoral Hernia Surgery Cost in Delhi
The cost of femoral hernia surgery in Delhi depends on five things:
- The technique — open repair is the most economical, laparoscopic is mid-range, robotic is at the top
- Whether it is elective or emergency — emergency strangulated repair includes ICU monitoring and longer stay
- The mesh used — standard polypropylene vs. mid-weight composite vs. self-fixing mesh
- The hospital category — NABH-accredited tertiary hospitals naturally cost more
- Your insurance coverage — cashless coverage typically covers most or all of the cost
Indicative price bands at our partner hospitals:
- Open McVay / Plug-and-Patch repair: starting from ₹50,000
- Laparoscopic TAPP / TEP repair: starting from ₹65,000
- Robotic femoral hernia repair: starting from ₹2,50,000
- Emergency strangulated femoral hernia repair: custom quote based on hospital stay and bowel resection requirement
We accept cashless insurance from all major Indian insurers, and we offer zero-interest EMI through our clinic partners. You will receive a transparent, fixed-price estimate before you commit — no hidden costs, no surprise bills on discharge day.
For a detailed breakdown, please read our complete guide: Cost of Hernia Surgery in Delhi.
Femoral Hernia Surgery Cost in Delhi
Get accurate cost estimate for your treatment
Why Patients Choose Dr. Kapil Agrawal for Femoral Hernia Surgery in Delhi
Dr. Kapil Agrawal brings internationally accredited surgical training (MRCS London, MMed Singapore) and 23+ years of laparoscopic and robotic hernia experience to every femoral hernia repair.
- Dedicated focus on female groin hernia — our outcomes are tracked, our complication rates are published, and our recurrence rate is below 2%
- All techniques under one surgeon — laparoscopic TAPP, TEP, robotic, and open McVay
- 24/7 emergency availability — strangulated femoral hernia is a true emergency, and we have on-call protocols at our partner hospitals
- Apollo Hospitals, Delhi NCR — Senior Consultant access at one of India's top hospital networks
- Female-friendly clinic environment — many of our femoral hernia patients prefer to be examined by a female assistant initially, and we accommodate this without any awkwardness
- Free lifetime follow-up — Dr. Agrawal personally reviews every patient at 1 week, 1 month, 3 months, and beyond, at no additional cost
- Transparent, fixed-price packages — including pre-op tests, anaesthesia, mesh, surgery, and post-op care
- Cashless insurance and zero-interest EMI
- Two convenient South Delhi clinics — Lajpat Nagar and Hauz Khas, easily reachable from Defence Colony, GK, Saket, Green Park, Vasant Kunj, South Extension, and CR Park
Habilite Clinics' Free Post-operative Care
We provide comprehensive free post-operative care to ensure your smooth recovery and optimal results. Our dedicated team is committed to your well-being throughout your healing journey.
Comprehensive Care
Complete post-operative support and monitoring
Expert Guidance
24/7 access to our medical team
Dedicated Support
Personalized care coordinator for each patient
Regular Follow-ups
Scheduled check-ups to ensure optimal recovery
What's Included in Our Free Post-operative Care:
- ✓Regular follow-up consultations with Dr. Kapil Agrawal
- ✓24/7 emergency support and guidance
- ✓Nutritional counseling and diet plans
- ✓Wound care and dressing assistance
- ✓Medication management and adjustments
- ✓Progress monitoring and recovery assessment
Chat with Expert for Free
Get instant answers to your questions from our medical experts via WhatsApp
Frequently Asked Questions
How is a femoral hernia different from an inguinal hernia?
Why is femoral hernia more common in women?
Can a femoral hernia be dangerous?
Is femoral hernia surgery painful?
How soon can I return to work and household activities?
Can a femoral hernia heal without surgery?
Is laparoscopic surgery suitable for femoral hernia in older women?
Can both groins be repaired in a single surgery if I have hernias on both sides?
Does femoral hernia surgery affect my future pregnancies?
What happens if I keep ignoring my femoral hernia?
Is femoral hernia surgery covered by health insurance in India?
My doctor told me my 'inguinal hernia' was repaired, but the bulge is back. Could it actually be a femoral hernia?
Do you offer emergency surgery for strangulated femoral hernia?
How long does femoral hernia surgery take?
Take the Next Step
If you have noticed a small but persistent bulge or tenderness on your upper inner thigh, please do not let anyone — including yourself — dismiss it as a 'muscle pull' Dismissing a groin bulge as a 'muscle pull' is one of the most common hernia myths I correct every week. or 'swollen gland'. Femoral hernia is a treatable, predictable condition when caught early — and a medical emergency when caught late.
I would be glad to see you, examine you, and walk you through your specific options.
- Call: +91 99994 56455 / +91 99100 24564
- WhatsApp: Share your symptoms
- Visit: Habilite Clinics, Lajpat Nagar (M-11, Block M) or Hauz Khas (C-7/186, SDA), New Delhi
Related Femoral Hernia Blogs
Expert insights, tips, and guides about femoral hernia
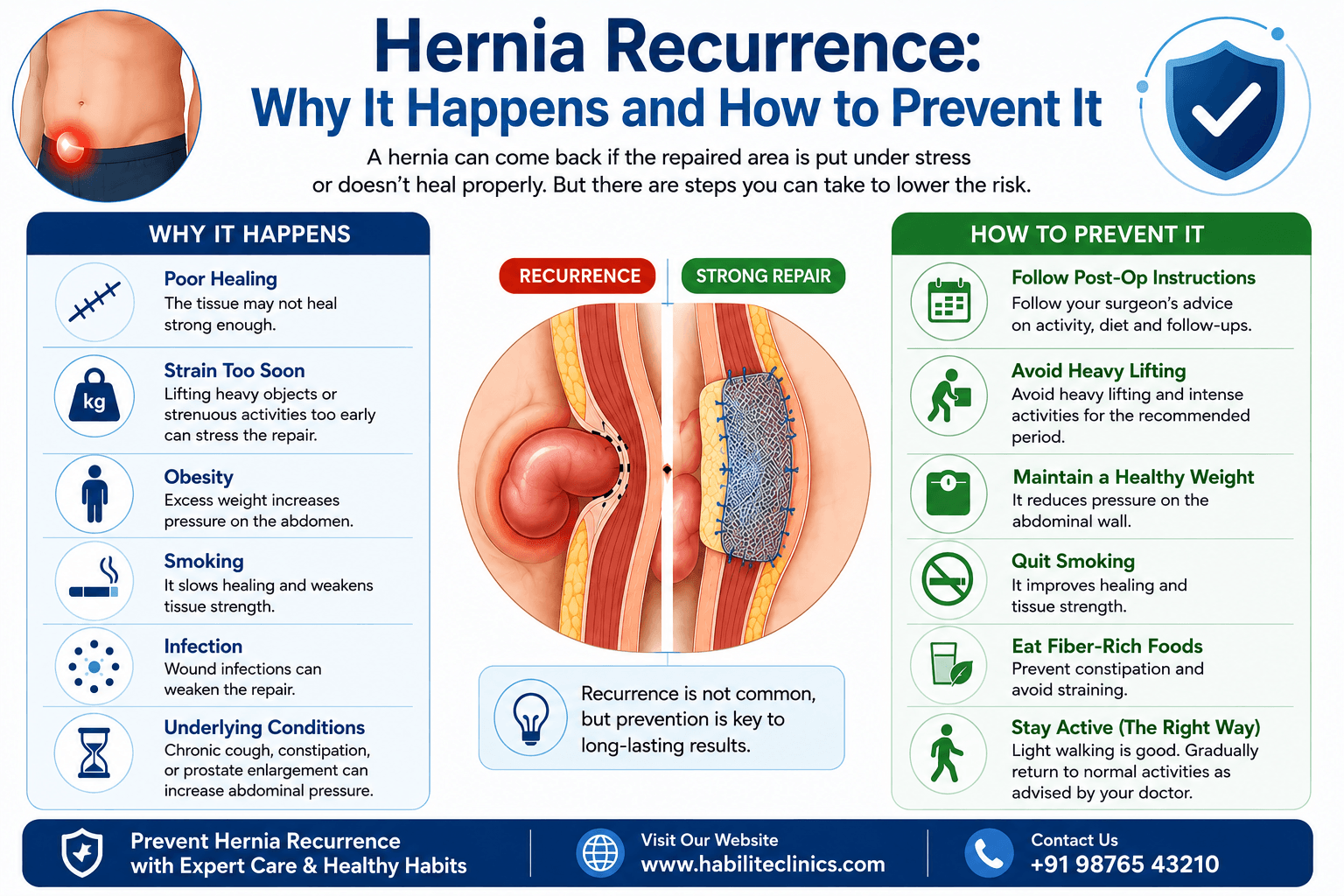
Hernia Recurrence: Why It Happens and How to Prevent It
You have been through a hernia surgery. The recovery was uncomfortable. You followed the doctor's advice. And now, months or even years later, you feel a familiar lump or twinge in exactly the same spot. A wave of worry washes over you.
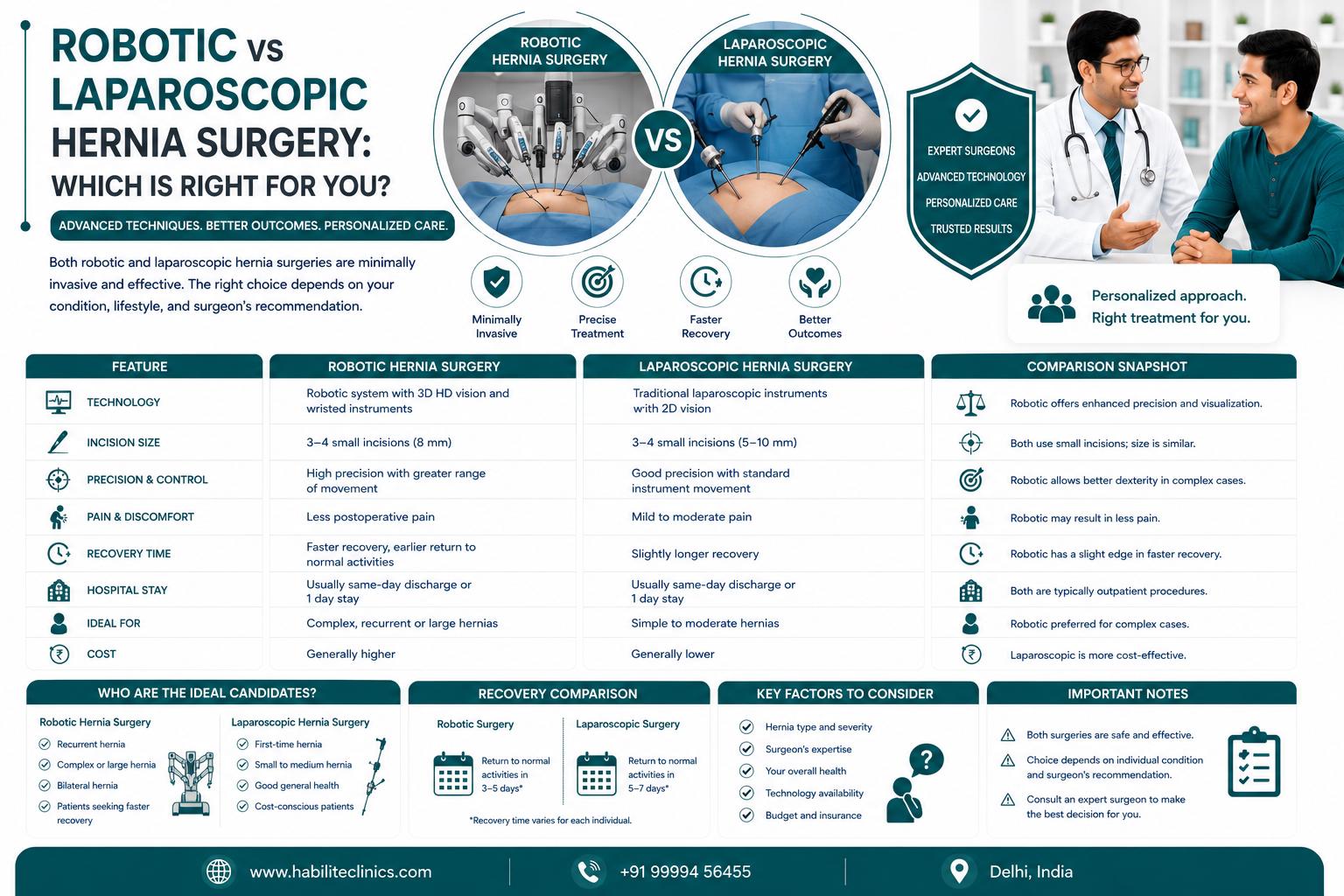
Robotic vs Laparoscopic Hernia Surgery: Which Is Right for You?
Both robotic and laparoscopic hernia surgeries are minimally invasive options with smaller cuts, less pain, and faster recovery than traditional open surgery. ✓ Robotic hernia surgery offers 3D high-definition vision, greater precision with 540-degree instrument rotation, and tremor filtration for complex cases. ✓ Laparoscopic surgery is more widely available, more affordable (₹40,000-50,000 less expensive), and equally effective for most standard hernias. ✓ Dr. Kapil Agrawal and our team at Habilite Clinics offer both techniques with 23+ years of surgical experience. ✓ The choice between robotic and laparoscopic depends on hernia type, complexity, prior surgeries, patient health, and cost considerations—not all patients need robotic surgery. ✓ Both procedures have been covered by health insurance in India since 2019 under IRDAI guidelines, making advanced minimally invasive surgery accessible to more patients.
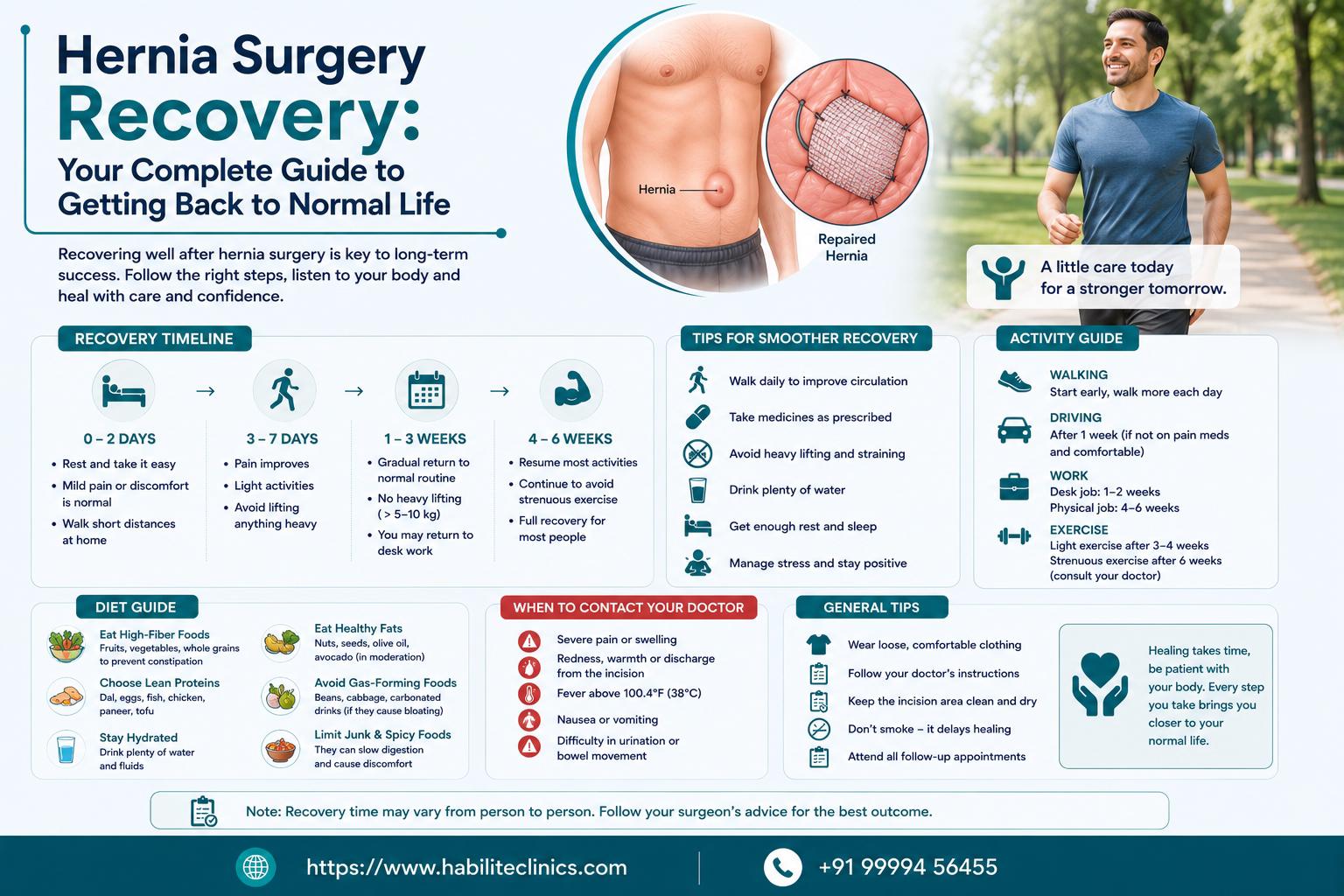
Hernia Surgery Recovery: Your Complete Guide to Getting Back to Normal Life
Recovery varies by surgery type: Laparoscopic hernia surgery recovery takes 1-2 weeks for light activities, while open surgery may need 4-6 weeks Early movement is essential: Walking within hours of surgery prevents blood clots and speeds healing. Complete bed rest is outdated and harmful You can eat normal food, use Indian toilets, and don't need months of rest after modern hernia surgery A protein-rich diet accelerates healing: Focus on eggs, dal, chicken, and fish to rebuild muscle strength after surgery Warning signs need immediate attention: Sudden severe pain, fever above 101°F, or inability to pass gas requires urgent medical care Return to work depends on your job: Desk jobs allow return in 1-2 weeks; manual labor jobs need 4-6 weeks recovery