
Best Hernia Surgeon in Delhi - Dr. Kapil Agrawal
If you or someone in your family has been told you need hernia surgery, you are probably asking the same question most of our patients ask us: who is the best hernia surgeon in Delhi, and how do I know I'm in the right hands? At Habilite Clinics, Dr. Kapil Agrawal has spent more than 23 years answering exactly that question — through careful consultations, patient-first surgery, and over 7,000 successful laparoscopic and robotic hernia repairs.
As a Senior Consultant Surgeon at Apollo Hospitals, Delhi NCR, Dr. Kapil Agrawal is widely regarded among patients and peers as one of the best hernia doctors in Delhi for complex, recurrent, and routine hernia cases alike. Our team offers the full spectrum of modern hernia treatment — open repair, laparoscopic (keyhole) repair, and robotic-assisted repair — and we choose the right technique for you, not the other way round.
Who is Dr. Kapil Agrawal — and Why Patients Call Him the Best Hernia Surgeon in Delhi?
We understand that choosing the best hernia surgeon in Delhi is not a decision you take lightly. Your surgeon's experience, training, hospital access, and judgement all decide whether your hernia is fixed once — or comes back in two years.
Dr. Kapil Agrawal brings a combination that is hard to match in Delhi NCR:

Dr. Kapil Agrawal is widely searched for as the best hernia doctor in Delhi, the best hernia surgeon near me (for patients across South, Central and East Delhi), and the best laparoscopic hernia surgeon in Delhi NCR.
Understanding Your Hernia: Why It Happens and Why It Matters
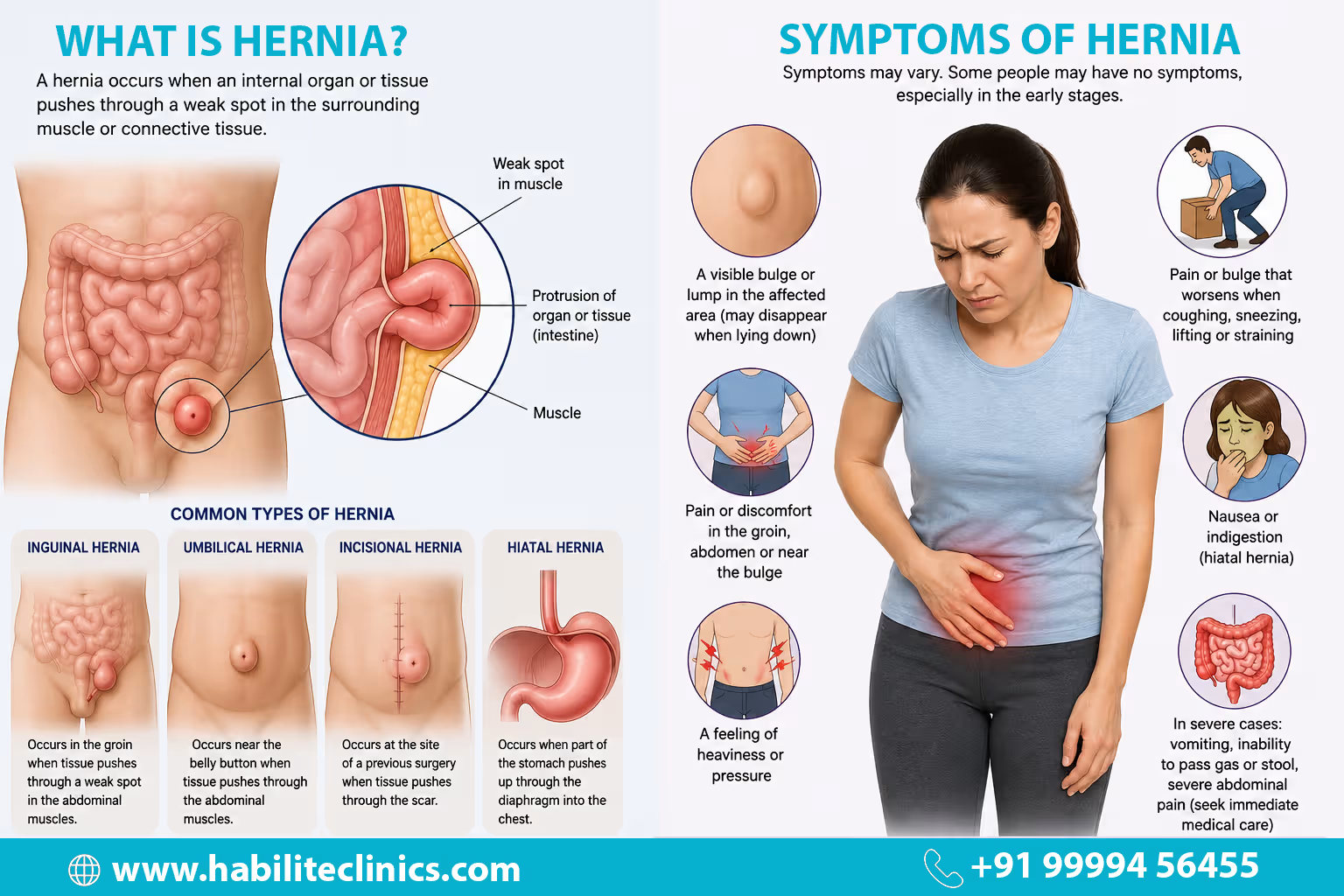
A hernia is a weakness or tear in the muscle wall of your abdomen through which internal tissue — often a loop of intestine or fat — pushes out and forms a visible bulge. Hernias do not heal on their own. They only get bigger with time, and a neglected hernia can become a surgical emergency if the tissue gets trapped (incarceration) or loses its blood supply (strangulation).
Common Symptoms of Hernia
- A visible bulge or swelling in the groin, navel, or surgical scar area
- Pain or pulling sensation, especially when lifting, coughing, or standing for long
- A feeling of heaviness, pressure, or dragging in the lower abdomen
- Burning, gurgling, or aching at the site of the bulge
- For hiatus hernias: acid reflux, heartburn, and chest discomfort after meals
When You Must See a Hernia Specialist Immediately
If your bulge suddenly becomes very painful, hard, or impossible to push back — or if it is accompanied by nausea, vomiting, or fever — please do not wait for an outpatient appointment. Call us, or go to the nearest emergency room. This may indicate a strangulated hernia, and the time to surgery matters.
Types of Hernia We Treat at Habilite Clinics
Dr. Kapil Agrawal and our team treat every category of abdominal wall hernia, from straightforward to deeply complex.
Inguinal Hernia
An inguinal hernia occurs in the groin when abdominal tissue pushes through a weak spot in the abdominal wall. It is more common in men and may cause pain or discomfort during physical activity.
Read more about Inguinal HerniaUmbilical Hernia
An umbilical hernia develops near the navel. While it is commonly seen in infants, it can also affect adults, especially those with obesity or repeated abdominal strain.
Read more about Umbilical HerniaIncisional Hernia
An incisional hernia forms at the site of a previous surgical scar. These hernias may enlarge over time and often require specialized surgical management.
Read more about Incisional HerniaHiatus Hernia
A hiatus hernia occurs when part of the stomach moves upward into the chest through the diaphragm. It may lead to symptoms such as acid reflux, heartburn, or chest discomfort.
Read more about Hiatus HerniaEpigastric Hernia
Epigastric hernia occurs between the umbilicus and the rib cage. Epigastric hernia presents as a bulge which is usually painful and progresses in size with time.
Read more about Epigastric HerniaFemoral Hernia
A femoral hernia appears near the upper thigh and is more commonly seen in women. It can be difficult to detect and carries a higher risk of complications such as strangulation.
Read more about Femoral HerniaSurgical Techniques We Offer
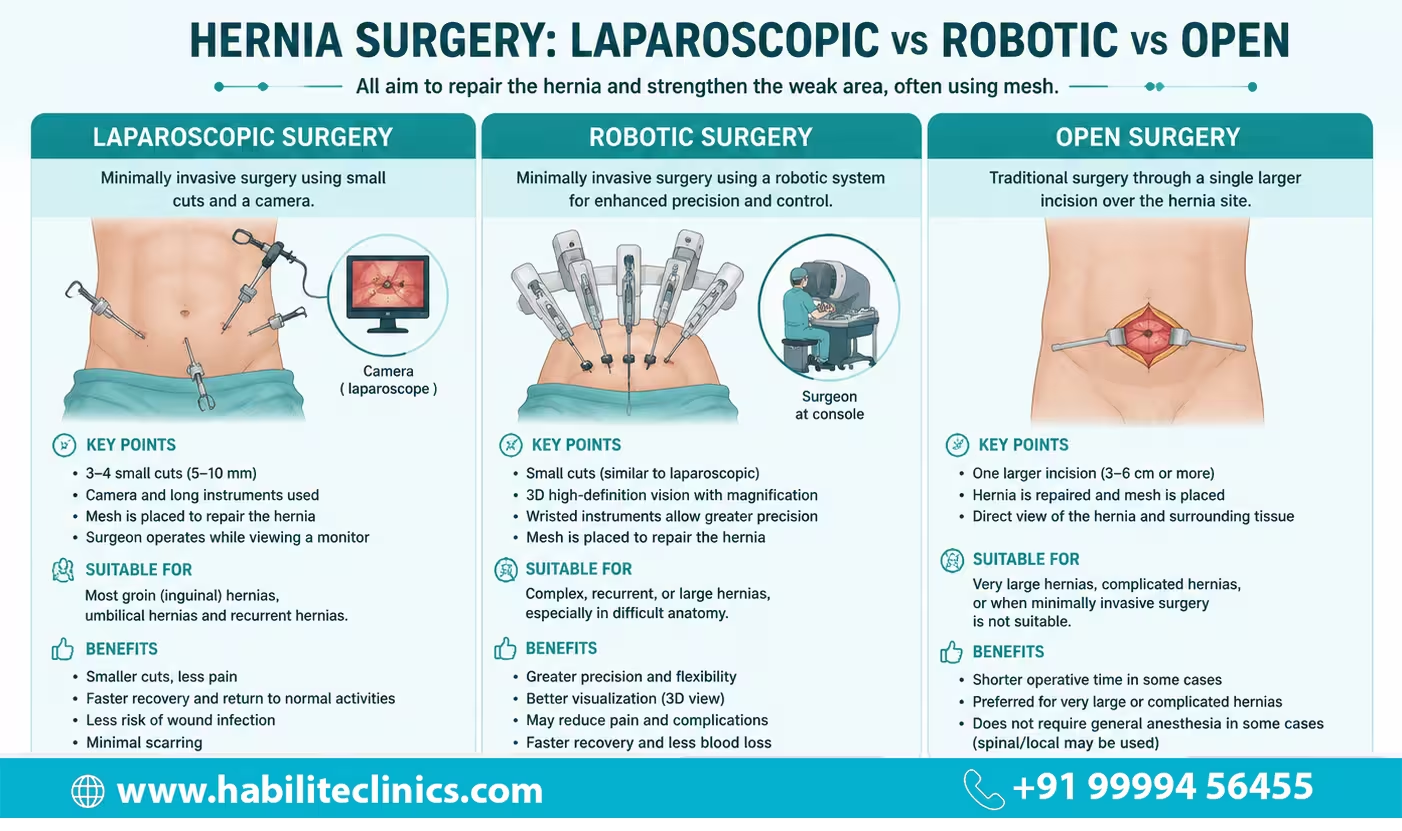
Laparoscopic Hernia Surgery in Delhi
For the vast majority of inguinal, umbilical, and small-to-medium ventral hernias, we recommend laparoscopic repair. Through 3–4 tiny incisions (5–10 mm), Dr. Kapil Agrawal places a high-definition camera and delicate instruments into your abdomen, and repairs the defect from behind the abdominal wall with a precisely fitted mesh.
What this means for you:
- Minimal visible scarring — most scars fade completely within a year
- Significantly less post-operative pain than open surgery
- Drastically lower risk of wound infection
- Most patients walk within 2 hours of surgery and go home the same day or within 24 hours
- Return to desk work in 7–10 days; full normal activity in 3–4 weeks
We routinely perform both TAPP (Transabdominal Pre-Peritoneal) and TEP (Totally Extra-Peritoneal) techniques — the two gold-standard approaches for laparoscopic inguinal hernia repair — as well as the newer eTEP (enhanced-view Totally Extra-Peritoneal) for appropriate ventral and incisional cases.
Robotic Hernia Surgery in Delhi
Robotic surgery is the most advanced platform available for hernia repair today, and Dr. Kapil Agrawal has built considerable experience with it for cases where precision truly changes the outcome.
From the robotic console, our surgeon controls wristed instruments with a range of motion that exceeds the human hand, while viewing your anatomy in magnified 3D high-definition. For large ventral hernias, recurrent hernias, and cases requiring abdominal wall reconstruction, this precision matters.
Key advantages for you:
- Superior mesh placement and fixation in difficult anatomy
- Safer dissection in scarred tissue from previous surgery
- Lower recurrence rates in complex cases as per published literature
- Same minimally invasive recovery as standard laparoscopy — small scars, early discharge
Open Hernia Surgery in Delhi
We are clear with our patients: laparoscopic and robotic are not always better. For some patients — very large hernias with loss of abdominal domain, severe prior adhesions, or specific medical contraindications to general anaesthesia — conventional open repair remains the safest and most durable option. When that is the case, we do open repair with the same meticulous care, reinforcing the defect with a tension-free mesh.
Advantages of Laparoscopic & Robotic Hernia Repair
How We Decide Which Hernia Surgery Is Right for You
One of the reasons patients refer their family and friends to us as the best hernia surgery clinic in Delhi is that we don't run an assembly line. Dr. Kapil Agrawal personally examines every patient and tailors the procedure to your hernia, your body, and your life.
Our Consultation Protocol
- Detailed history and examination — we take the time to understand not just your hernia, but your work, your lifestyle, your diabetes control, your smoking status, and your recovery goals.
- Advanced imaging when needed — high-resolution ultrasound, or CT with 3D reconstruction for large or recurrent hernias, to map the exact defect.
- Shared decision-making — we explain every suitable option (open, laparoscopic, or robotic), the honest pros and cons of each, and help you choose.
- Pre-operative optimisation — if your BMI, sugars, or blood pressure need work before surgery, we partner with our nutritionists and physicians to get you ready.
Specialized Care for Complex & Recurrent Hernias
This is where choosing the best hernia surgeon in Delhi truly matters. Many of our patients come to us after a previous hernia repair has failed, or after being told elsewhere that their hernia is "too big" or "too complicated."
When Is a Hernia Classified as Complex?
- Defect wider than 10 cm, or with significant loss of abdominal domain
- Recurrent hernia after one or more prior repairs
- Incisional hernia after multiple abdominal surgeries
- Hernia with infected mesh from previous surgery
- Patients with morbid obesity, uncontrolled diabetes, COPD, or heart disease
Our Complex-Hernia Protocol
Our dedicated multi-disciplinary team follows a step-wise protocol:
Preoperative Optimization
We work with you over 4–8 weeks to lose weight, control your sugars, stop smoking, and build respiratory fitness — because this changes outcomes more than the surgery itself.
3D CT Planning
Every complex case is planned on a 3D CT reconstruction. We measure the defect, map muscle quality, and plan the operation before we enter the operating room.
Component Separation (TAR / ACS): For large midline defects, our team performs Transversus Abdominis Release (TAR) and anterior component separation to bring the abdominal wall muscles back to the midline without tension. This is the most physiological, durable repair available today for large ventral hernias.
Robotic abdominal wall reconstruction: Where appropriate, we perform the TAR repair robotically — gaining precision in a complex dissection that open surgery cannot match.
Multidisciplinary aftercare: Nutritionists, physiotherapists, pulmonologists, and endocrinologists work with our surgical team so your recovery isn't just about the scar — it's about returning you to full function.
Robotic Repair for Complex Abdominal Wall Hernias
Dr. Kapil Agrawal has vast experience dealing with complex abdominal wall hernias. He, along with his team, performs complex abdominal wall hernia repair using Robot-Assisted Laparoscopic Surgery. The 3D vision and wristed instruments, along with his expertise, allow him to navigate scarred anatomy with greater safety and precision.
Surgical Mesh: What You Should Know Before Surgery
Almost every modern hernia repair uses surgical mesh — a soft, flexible reinforcement that dramatically lowers the chance of the hernia coming back. Meshes vary in material (polypropylene, polyester, biologic, composite), weight (light, mid, heavy), and pore size. There is no single "best" mesh — the best mesh is the one that matches your hernia, your tissue, and your placement plane.
Our team selects mesh based on hernia type, location, size, your weight, your infection risk, and whether the mesh will contact bowel. We use internationally validated meshes only, and we explain to every patient which mesh we are placing and why.
Why Choose Habilite Clinics and Dr. Kapil Agrawal
- Transparent, fixed-price packages. No hidden costs, no surprise mesh bills. We give you a clear cost estimate before surgery, including insurance coordination and zero-interest EMI options.
- Free lifetime follow-up. Every patient of ours gets complimentary post-operative consultations with Dr. Agrawal, nutritional counselling, wound care, and 24/7 access to our medical team during recovery.
- South Delhi locations. Our clinics at Lajpat Nagar (M-11, Block M) and Hauz Khas (C-7/186, SDA) make us easily accessible if you've been searching best hernia surgeon near me from Defence Colony, Greater Kailash, Saket, Green Park, Vasant Kunj, South Extension, CR Park, or anywhere across South and Central Delhi.
Cost of Hernia Surgery in Delhi
The cost of hernia surgery in Delhi depends on the type of hernia (inguinal vs ventral vs incisional), the technique (open, laparoscopic, or robotic), the hospital category, your choice of mesh, and your insurance coverage.
Typical range at our partner hospitals:
- Laparoscopic inguinal hernia repair: Our package starts from ₹60,000
- Laparoscopic ventral/umbilical hernia repair: Our package starts from ₹60,000
- Robotic complex hernia / abdominal wall reconstruction: Our package starts from ₹2,50,000
We offer cashless insurance coordination with all major Indian insurers and zero-interest EMI options through our clinic partners. For a detailed breakdown, read our full guide: Cost of Hernia Surgery in Delhi.
What Recovery Looks Like After Your Hernia Surgery
Within 2 hours of surgery: You are awake, walking, and having sips of water.
Within 24 hours: You go home (same-day discharge for most non-insurance patients; 24-hour stay for insurance cashless cases).
Days 2–3: Resume your regular home diet as per your customized plan. Walking is encouraged, lifting is not.
Days 7–10: Most patients return to desk work and driving.
Weeks 3–4: Resume gym and moderate workouts as cleared in follow-up.
Week 6 onwards: Full return to heavy lifting, running, and all normal activities.
Our team gives every patient a written recovery blueprint, diet plan, and a dedicated care coordinator who stays in touch with you through the entire healing period — at no additional cost.
The Habilite Clinics Experience: Your Journey from Pain to Relief
Step-by-Step: From Your First Consultation to Full Recovery
Your journey begins with a detailed consultation and creation of a personalized surgical plan. On surgery day, our dedicated team ensures your complete comfort and safety. After your surgery, we provide a structured recovery blueprint, including diet, activity guidelines, and physiotherapy.
World-Class Facilities: Surgery at Premium Hospitals with Advanced Technology
We perform surgery at Delhi NCR's premier hospitals. We always ensure the highest global standards of safety, hygiene, and nursing care. These hospitals are equipped with the latest generation technology including advanced 3D/4K laparoscopic systems and the Robotic system.
Transparent Planning: Clear Cost Estimates, Insurance & EMI Assistance
The cost of hernia surgery in Delhi can vary depending on the type of hernia, the kind of surgery (open, laparoscopic, or robotic), and the hospital and facilities.
Laparoscopic and robotic surgeries tend to cost more, but they also offer faster healing, smaller scars, and less pain.
Dr. Kapil Agrawal's clinic offers clear pricing with insurance support and cost-effective packages, so you know exactly what you're paying for.
Our clinic partners also offer zero-interest EMI options.
Hernia Patient Testimonials
Real stories from patients who underwent laparoscopic and robotic hernia repair with Dr. Kapil Agrawal
Patient testimonial about hernia surgery experience with Dr. Kapil Agrawal.
Hernia Surgery Patient
Hernia Surgery
Patient testimonial about hernia surgery experience with Dr. Kapil Agrawal.
Hernia Surgery Patient
Hernia Surgery
Patient testimonial about hernia surgery experience with Dr. Kapil Agrawal.
Hernia Surgery Patient
Hernia Surgery
Habilite Clinics' Free Post-operative Care
We provide comprehensive free post-operative care to ensure your smooth recovery and optimal results. Our dedicated team is committed to your well-being throughout your healing journey.
Comprehensive Care
Complete post-operative support and monitoring
Expert Guidance
24/7 access to our medical team
Dedicated Support
Personalized care coordinator for each patient
Regular Follow-ups
Scheduled check-ups to ensure optimal recovery
What's Included in Our Free Post-operative Care:
- ✓Regular follow-up consultations with Dr. Kapil Agrawal
- ✓24/7 emergency support and guidance
- ✓Nutritional counseling and diet plans
- ✓Wound care and dressing assistance
- ✓Medication management and adjustments
- ✓Progress monitoring and recovery assessment
Frequently Asked Questions
Everything you need to know about hernia symptoms, treatment, recovery, and insurance
Who is the best hernia surgeon in Delhi?
Dr. Kapil Agrawal is widely regarded as one of the best hernia surgeons in Delhi NCR, with over 23 years of experience, 7,000+ hernia surgeries performed, and a Senior Consultant position at Apollo Hospitals. He specializes in laparoscopic, robotic, and complex abdominal wall reconstruction for both routine and recurrent hernias.
How do I choose the best hernia doctor in Delhi for my case?
Look for a surgeon who performs hernia repair as a primary specialty (not as an occasional procedure), has documented volume in both laparoscopic and robotic techniques, operates at an accredited hospital, gives you a detailed consultation before surgery, and offers transparent pricing. At Habilite Clinics, Dr. Kapil Agrawal offers all of these as standard.
What is the cost of hernia surgery in Delhi?
The cost of hernia surgery in Delhi typically ranges from ₹75,000 for a straightforward laparoscopic inguinal repair to ₹4,00,000 for complex robotic abdominal wall reconstruction. Cost depends on hernia type, surgical technique, hospital, and mesh used. We provide transparent cost estimates with full insurance and EMI support.
Is laparoscopic hernia surgery safe?
Yes. Laparoscopic hernia repair is the gold-standard, minimally invasive treatment for most hernias. It has a success rate above 95%, minimal post-operative pain, and allows same-day discharge for most patients. Complications are rare and our team is trained to manage them immediately if they arise.
How long does it take to recover from hernia surgery?
After laparoscopic or robotic hernia repair, most of our patients return to desk work within 7–10 days and to full physical activity within 3–4 weeks. Open or complex repairs take 4–6 weeks to full recovery. Dr. Kapil Agrawal gives every patient a personalized recovery plan.
Can a hernia heal without surgery?
No. A hernia is a structural defect in the muscle wall and cannot close on its own. Belts, exercises, and diet may temporarily reduce discomfort, but the only permanent treatment is surgical repair by a qualified hernia surgeon.
Is hernia surgery covered by insurance in India?
Yes. Nearly all health insurance policies in India cover hernia surgery as a medically necessary procedure. Habilite Clinics offers complete cashless coordination with major insurers and can help you understand your exact coverage before surgery.
What is the best hospital for hernia surgery in Delhi?
Dr. Kapil Agrawal operates at Apollo Hospitals and other top-tier NABH-accredited facilities across Delhi NCR. These hospitals offer the latest 3D/4K laparoscopic systems, robotic surgery platforms, and full critical-care support — giving you the safety of a tertiary hospital with the personal attention of a private surgical practice.
Which is better — laparoscopic, robotic, or open hernia surgery?
For most patients, laparoscopic hernia surgery is the right answer — it offers minimal pain, tiny scars, and rapid recovery. Robotic surgery is preferred for complex, large, or recurrent hernias where precision matters. Open surgery is reserved for specific cases where minimally invasive techniques are not suitable. Dr. Kapil Agrawal will recommend the right technique for your hernia.
Do you offer consultations for hernia patients outside Delhi?
Yes. We offer video consultations for patients across India and internationally, and our international patient desk coordinates travel, accommodation, and complete hernia treatment packages in Delhi.
Related Hernia Blogs
Expert insights, tips, and guides about hernia
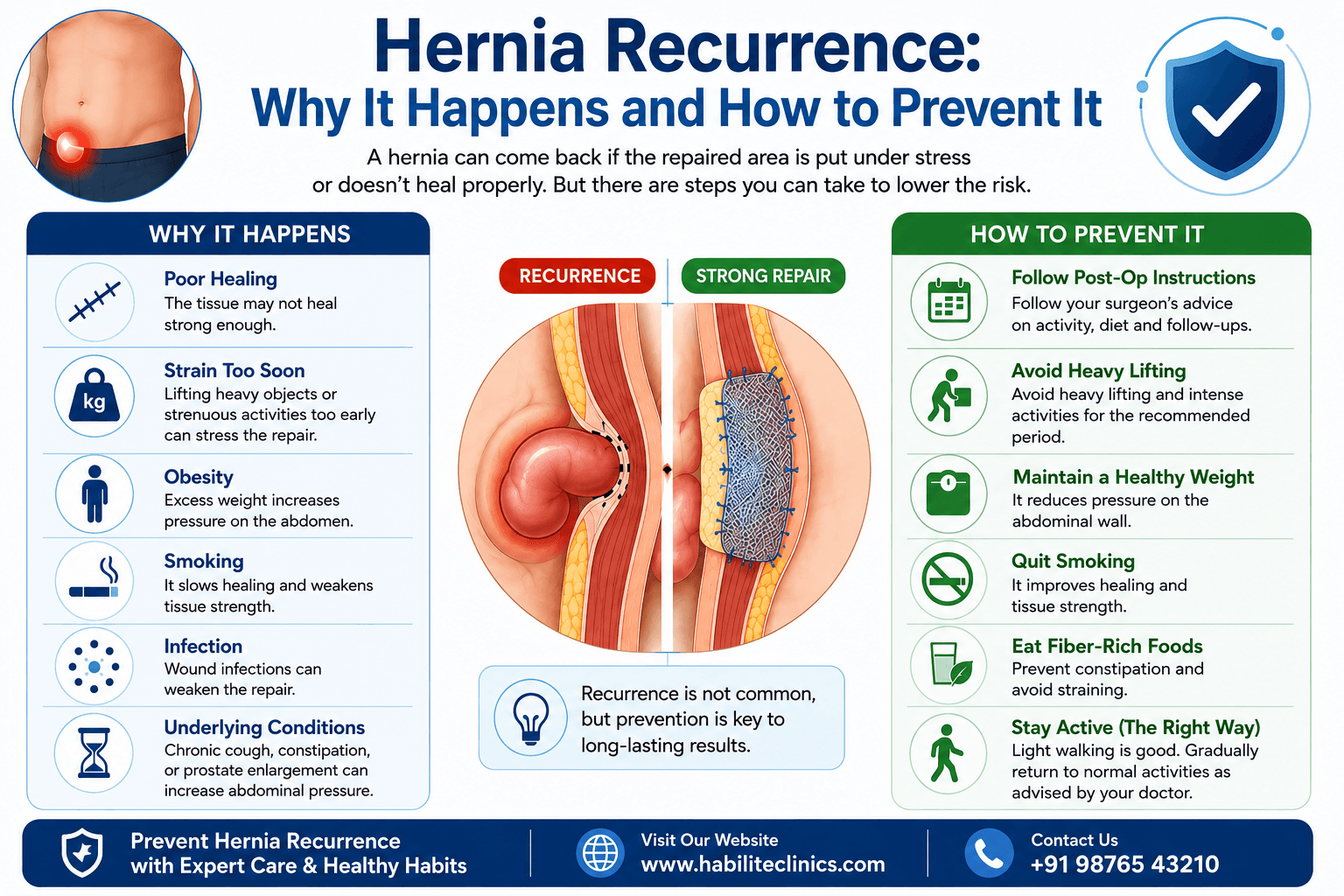
Hernia Recurrence: Why It Happens and How to Prevent It
You have been through a hernia surgery. The recovery was uncomfortable. You followed the doctor's advice. And now, months or even years later, you feel a familiar lump or twinge in exactly the same spot. A wave of worry washes over you.
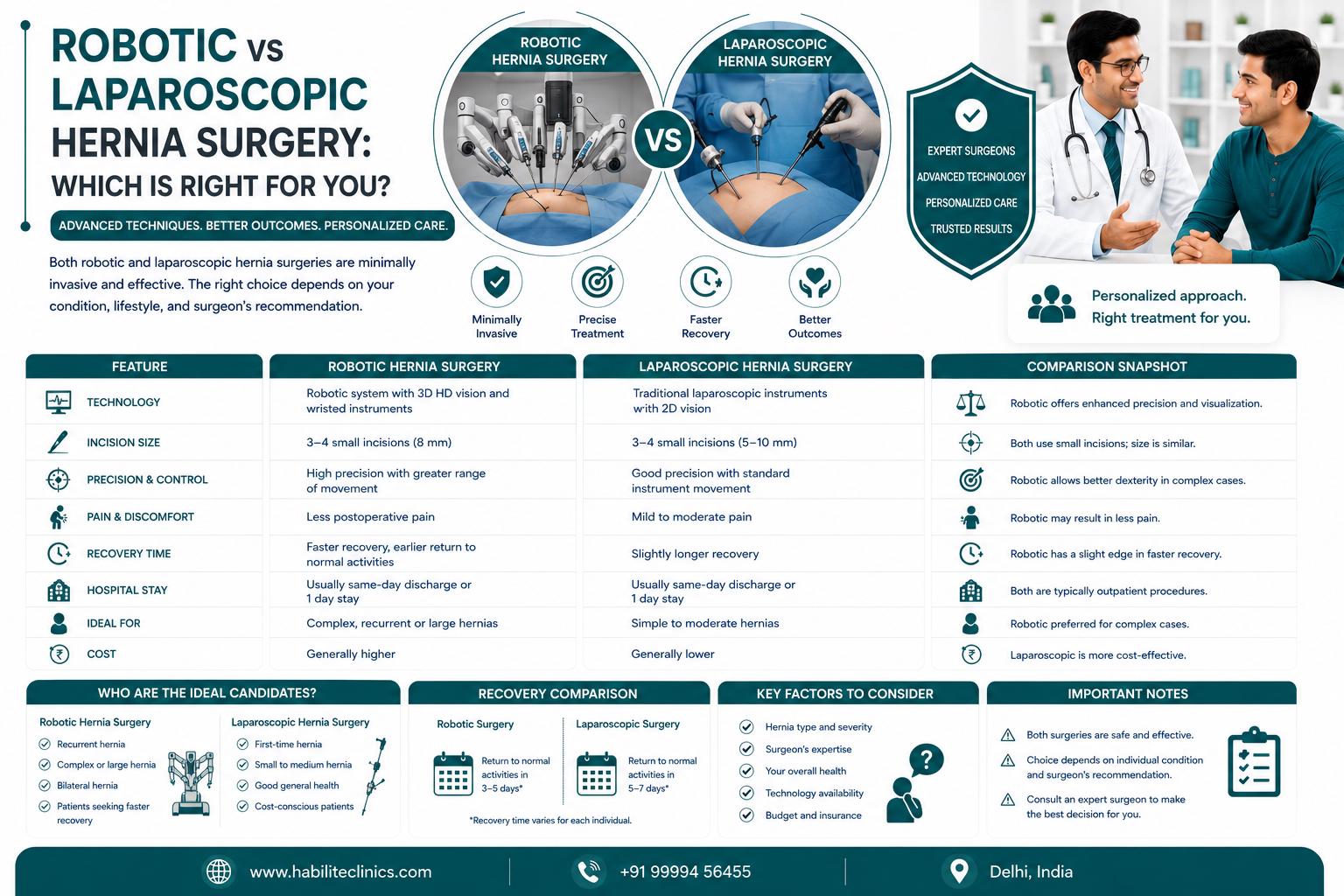
Robotic vs Laparoscopic Hernia Surgery: Which Is Right for You?
Both robotic and laparoscopic hernia surgeries are minimally invasive options with smaller cuts, less pain, and faster recovery than traditional open surgery. ✓ Robotic hernia surgery offers 3D high-definition vision, greater precision with 540-degree instrument rotation, and tremor filtration for complex cases. ✓ Laparoscopic surgery is more widely available, more affordable (₹40,000-50,000 less expensive), and equally effective for most standard hernias. ✓ Dr. Kapil Agrawal and our team at Habilite Clinics offer both techniques with 23+ years of surgical experience. ✓ The choice between robotic and laparoscopic depends on hernia type, complexity, prior surgeries, patient health, and cost considerations—not all patients need robotic surgery. ✓ Both procedures have been covered by health insurance in India since 2019 under IRDAI guidelines, making advanced minimally invasive surgery accessible to more patients.
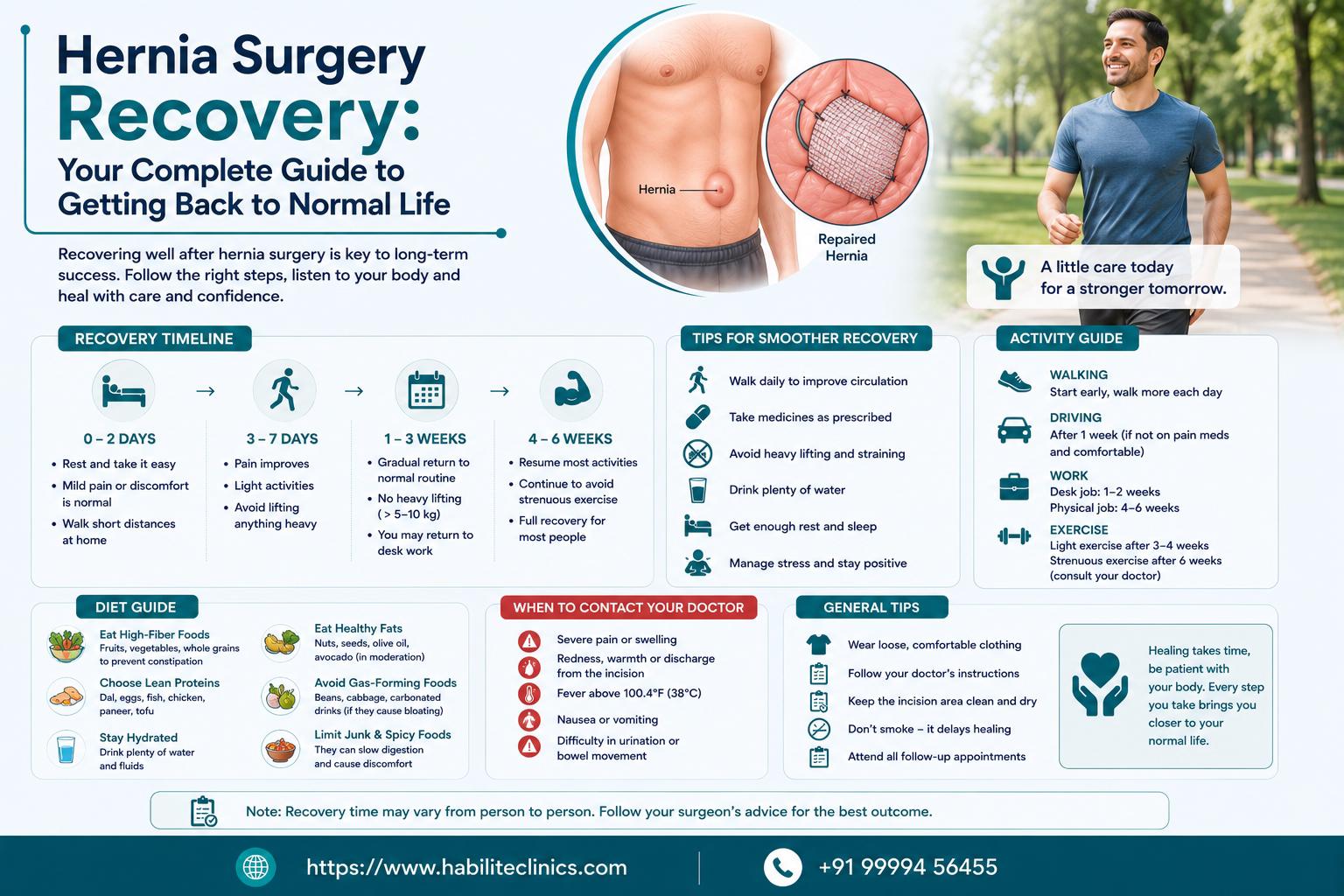
Hernia Surgery Recovery: Your Complete Guide to Getting Back to Normal Life
Recovery varies by surgery type: Laparoscopic hernia surgery recovery takes 1-2 weeks for light activities, while open surgery may need 4-6 weeks Early movement is essential: Walking within hours of surgery prevents blood clots and speeds healing. Complete bed rest is outdated and harmful You can eat normal food, use Indian toilets, and don't need months of rest after modern hernia surgery A protein-rich diet accelerates healing: Focus on eggs, dal, chicken, and fish to rebuild muscle strength after surgery Warning signs need immediate attention: Sudden severe pain, fever above 101°F, or inability to pass gas requires urgent medical care Return to work depends on your job: Desk jobs allow return in 1-2 weeks; manual labor jobs need 4-6 weeks recovery